

Calcium Channel Blocker Versus Renin-Angiotensin System Inhibitor in Risk of Kidney Cancer Among Patients With Hypertension: A Propensity Score-Matched Cohort Study
- PMID: 39548764
- PMCID: PMC11568363
- DOI: 10.1002/cam4.70429
Calcium Channel Blocker Versus Renin-Angiotensin System Inhibitor in Risk of Kidney Cancer Among Patients With Hypertension: A Propensity Score-Matched Cohort Study
Abstract
Background: Use of antihypertensive medications could be associated with an increased risk of kidney cancer. Despite their various mechanisms of action, whether this association differs between different classes of medications remains unclear.
Objective: The objective of this study is to compare the risk of kidney cancer between first-line treatment options of antihypertensive medications in a hypertensive population.
Method: In this retrospective cohort study, we used the MarketScan Databases (2007-2021). We included individuals older than 30 years of age with a diagnosis of hypertension who received first-line medications for hypertension, which included three classes: angiotensin-converting enzyme inhibitors (ACEI), angiotensin receptor blockers (ARB), and dihydropyridine calcium channel blockers (dCCB). We applied a propensity score matching method and created three separate cohorts: (1) ARB versus ACEI, (2) dCCB versus ACEI, and (3) dCCB versus ACEI. For non-dCCB, we repeated the analyses. The primary outcome was kidney cancer incidence. To assess kidney cancer risk, we applied multivariable conditional Cox proportional hazards models.
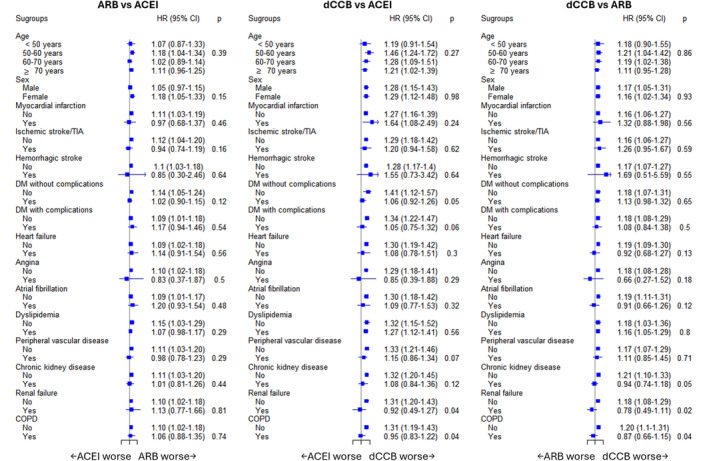
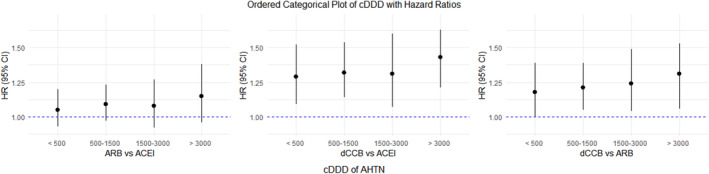
Results: In the first cohort, ARB use was associated with an increased risk of kidney cancer compared to ACEI use (hazard ratio [HR] 1.10, 95% confidence interval [CI] 1.02-1.18). In the second cohort, dCCB use was associated with an increased risk of kidney cancer compared to ACEI use (HR 1.29, 95% CI 1.18-1.40). In the third cohort, dCCB use was associated with a higher risk of kidney cancer compared to ARB use (HR 1.17, 95% CI 1.08-1.28). Null association was shown when comparing non-dCCB with ACEI or ARB use.
Conclusion: Use of dCCB showed a higher risk of kidney cancer compared to ACEI or ARB use in patients with hypertension.
Keywords: antihypertensive drugs; calcium channel blocker; hypertension; kidney cancer; renin–angiotensin system inhibitor.
© 2024 The Author(s). Cancer Medicine published by John Wiley & Sons Ltd.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
Similar articles
-
Angiotensin Receptor Blockers for Hypertension and Risk of Epilepsy.JAMA Neurol. 2024 Aug 1;81(8):866-874. doi: 10.1001/jamaneurol.2024.1714. JAMA Neurol. 2024. PMID: 38884986 Free PMC article.
-
Renin-angiotensin-aldosterone system inhibitors and SARS-CoV-2 infection: an analysis from the veteran's affairs healthcare system.Am Heart J. 2021 Oct;240:46-57. doi: 10.1016/j.ahj.2021.06.004. Epub 2021 Jun 12. Am Heart J. 2021. PMID: 34126079 Free PMC article.
-
Association of Inpatient Use of Angiotensin-Converting Enzyme Inhibitors and Angiotensin II Receptor Blockers With Mortality Among Patients With Hypertension Hospitalized With COVID-19.Circ Res. 2020 Jun 5;126(12):1671-1681. doi: 10.1161/CIRCRESAHA.120.317134. Epub 2020 Apr 17. Circ Res. 2020. PMID: 32302265 Free PMC article.
-
The use of renin-angiotensin-aldosterone system (RAAS) inhibitors is associated with a lower risk of mortality in hypertensive COVID-19 patients: A systematic review and meta-analysis.J Med Virol. 2021 Mar;93(3):1370-1377. doi: 10.1002/jmv.26625. Epub 2020 Nov 10. J Med Virol. 2021. PMID: 33095513
-
First-line drugs inhibiting the renin angiotensin system versus other first-line antihypertensive drug classes for hypertension.Cochrane Database Syst Rev. 2018 Nov 14;11(11):CD008170. doi: 10.1002/14651858.CD008170.pub3. Cochrane Database Syst Rev. 2018. Update in: Cochrane Database Syst Rev. 2023 Jul 13;7:CD008161. doi: 10.1002/14651858.CD008161.pub3. PMID: 30480768 Free PMC article. Updated.
Cited by
-
Association between antihypertensive medication use and kidney cancer risk: a meta-analysis accounting for hypertension.BMC Cancer. 2025 Jun 6;25(1):1013. doi: 10.1186/s12885-025-14406-3. BMC Cancer. 2025. PMID: 40481406 Free PMC article.
References
-
- National Cancer Institute , “Surveillance, Epidemiology, and End Results Program.” Cancer Stat Facts: Kidney and Renal Pelvis Cancer, accessed May 29, 2023, https://seer.cancer.gov/statfacts/html/kidrp.html.
-
- National Cancer Institute , “Annual Report to the Nation 2022: Overall Cancer Statistics.” Surveillance, Epidemiology, and End Results Program, accessed June 23, 2023, https://seer.cancer.gov/report_to_nation/statistics.html.
-
- American Cancer Society , “American Cancer Society: Cancer Facts and Figures 2022,” https://www.cancer.org/cancer/kidney‐cancer. Updated 2022.
-
- Cohen H. T. and McGovern F. J., “Renal‐Cell Carcinoma,” New England Journal of Medicine 353, no. 23 (2005): 2477–2490. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
