

Molecular Heterogeneity and Immune Infiltration Drive Clinical Outcomes in Upper Tract Urothelial Carcinoma
- PMID: 39550333
- PMCID: PMC12092068
- DOI: 10.1016/j.eururo.2024.10.024
Molecular Heterogeneity and Immune Infiltration Drive Clinical Outcomes in Upper Tract Urothelial Carcinoma
Abstract
Background and objective: Molecular classification of upper tract urothelial carcinoma (UTUC) can provide insight into divergent clinical outcomes and provide a biological rationale for clinical decision-making. As such, we performed multi-omic analysis of UTUC tumors to identify molecular features associated with disease recurrence and response to immune checkpoint blockade (ICB).
Methods: Targeted DNA and whole transcriptome RNA sequencing was performed on 100 UTUC tumors collected from patients undergoing nephroureterectomy. Consensus non-negative matrix factorization was used to identify molecular clusters associated with clinical outcomes. Gene set enrichment and immune deconvolution analyses were performed. Weighted gene co-expression network analysis was employed for unsupervised identification of gene networks in each cluster.
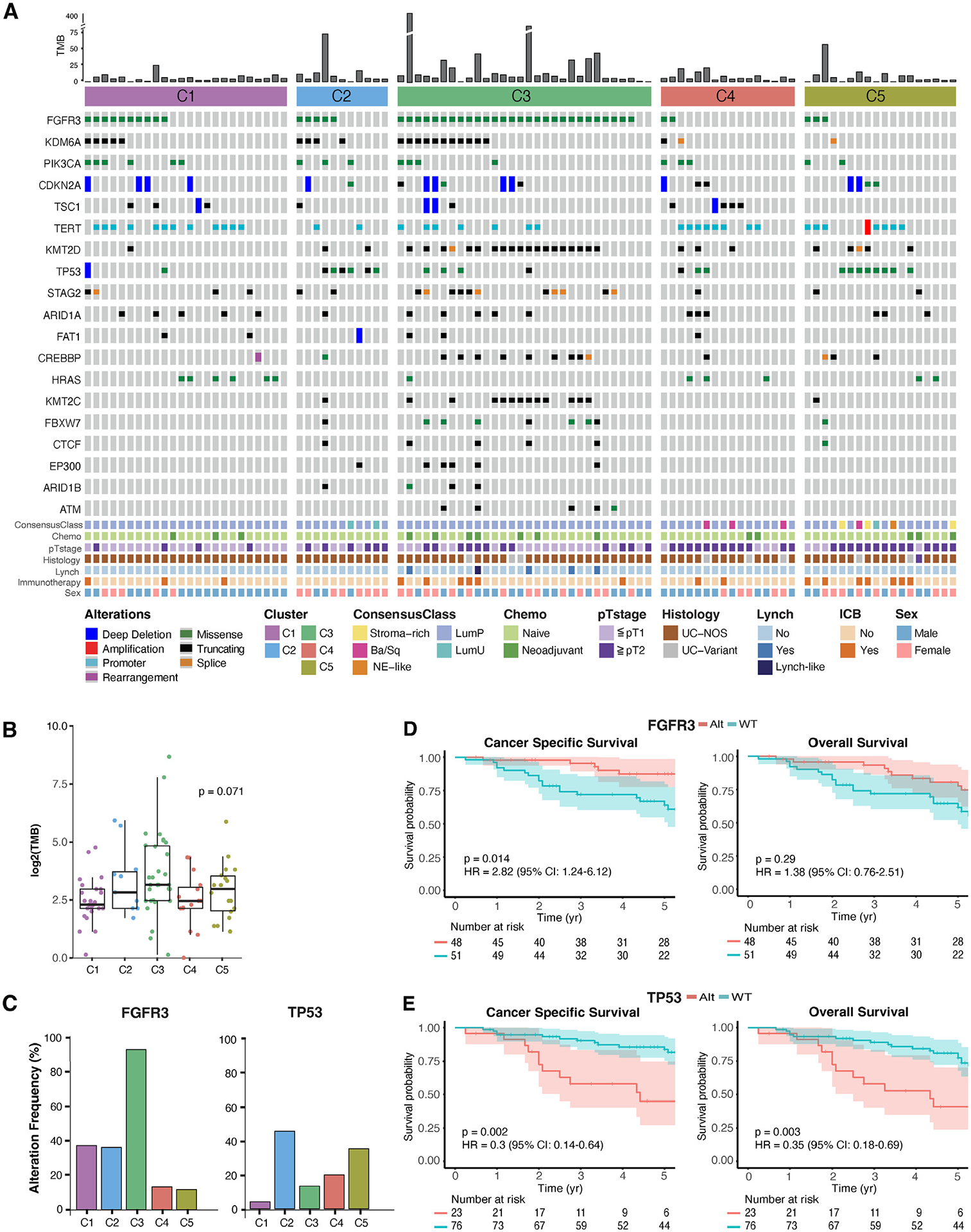
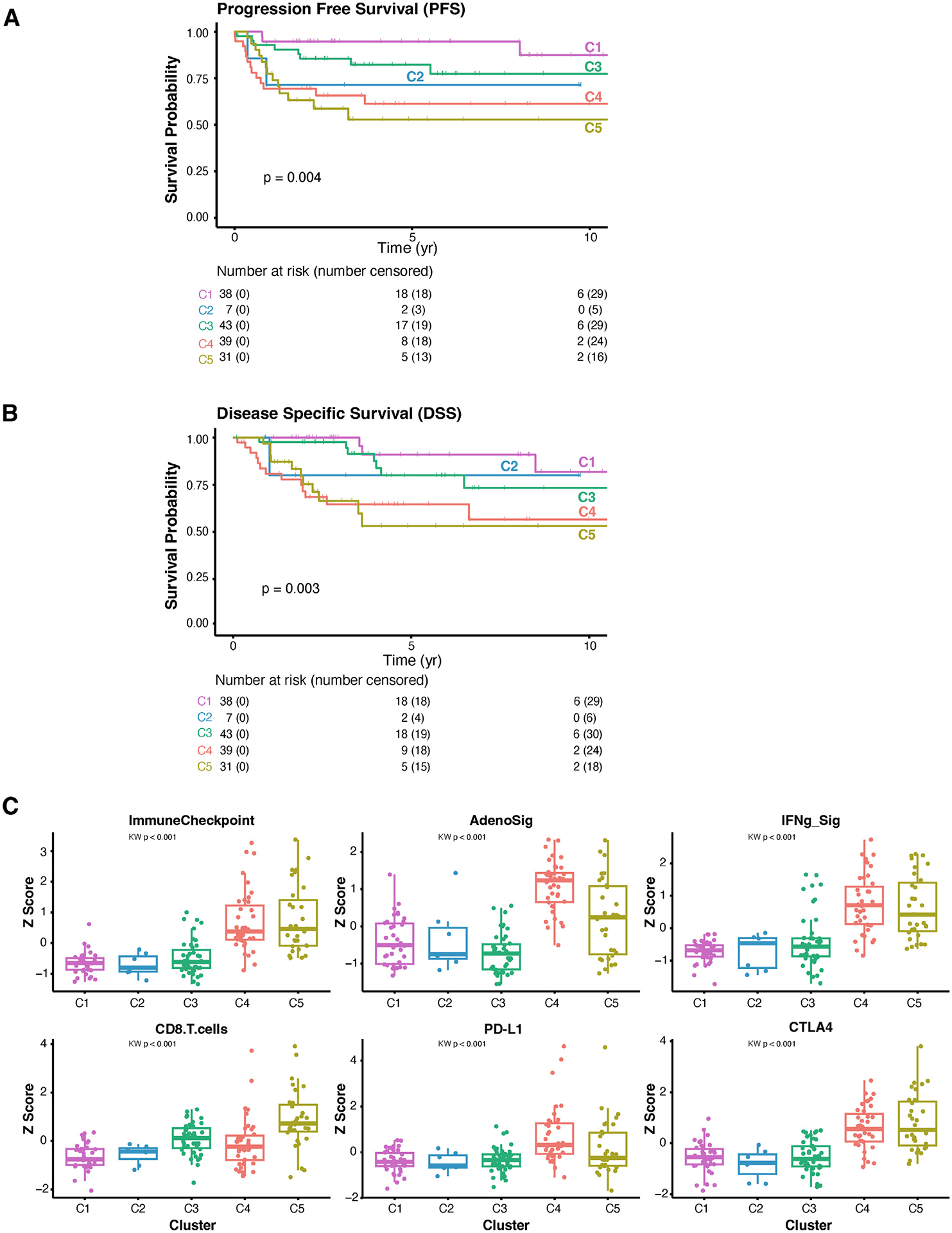
Key findings and limitations: Five molecular clusters with distinct clinical outcomes were identified. Favorable subtypes (C1 and C2) were characterized by a luminal-like signature and an immunologically depleted tumor microenvironment (TME). Subtype C3 was characterized by FGFR3 alterations and a higher tumor mutational burden, and included all tumors with microsatellite instability. Despite higher rates of recurrence and inferior survival, subtypes C4 and C5 harbored an immunologically rich TME favoring response to ICB. Limitations include extrapolation of molecular features of tumors from the primary site to determine response to systemic immunotherapy and the limited resolution of bulk sequencing to distinguish gene expression in the tumor, stroma, and immune compartments.
Conclusions and clinical implications: RNA sequencing identified previously underappreciated UTUC molecular heterogeneity and suggests that UTUC patients at the highest risk of metastatic recurrence following surgery include those most likely to benefit from perioperative ICB.
Keywords: Immune checkpoint blockade; Molecular clusters; Targeted exome sequencing; Tumor microenvironment; Upper tract urothelial cancer; Whole transcriptomic sequencing.
Copyright © 2024 The Authors. Published by Elsevier B.V. All rights reserved.
Figures



References
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
