

Kidney Outcomes in Transthyretin Amyloid Cardiomyopathy
- PMID: 39550765
- PMCID: PMC11571068
- DOI: 10.1001/jamacardio.2024.4578
Kidney Outcomes in Transthyretin Amyloid Cardiomyopathy
Abstract
Importance: Transthyretin amyloid cardiomyopathy (ATTR-CM) is a progressive cardiomyopathy that commonly presents with concomitant chronic kidney disease. Chronic kidney dysfunction is associated with worse outcomes, but the prognostic value of changes in kidney function over time has yet to be defined.
Objective: To assess the prognostic importance of a decline in estimated glomerular filtration rate (eGFR) in a large cohort of patients with ATTR-CM.
Design, setting, and participants: This retrospective, observational, single-center cohort study evaluated patients diagnosed with ATTR-CM at the National Amyloidosis Centre (NAC) in the UK who underwent an eGFR baseline assessment and a follow-up assessment at 1 year between January 2000 and April 2024. Data analysis was performed in June 2024.
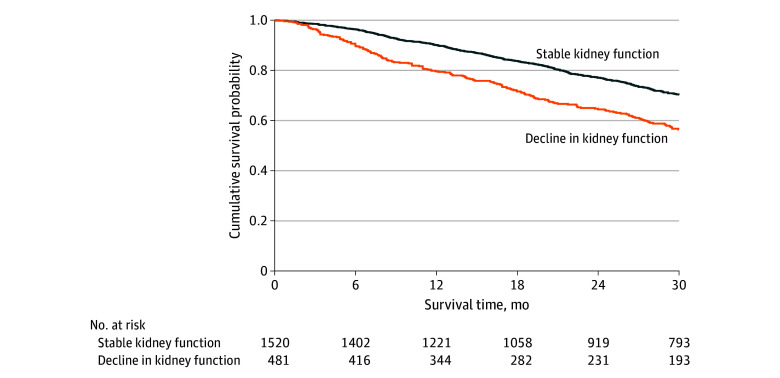
Main outcomes and measures: The primary outcome was the risk of all-cause mortality associated with decline in kidney function (defined as a decrease in eGFR >20%).
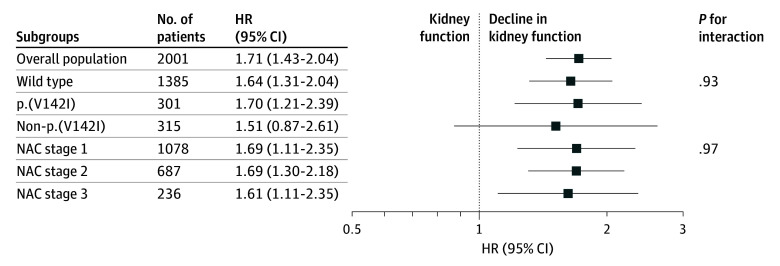
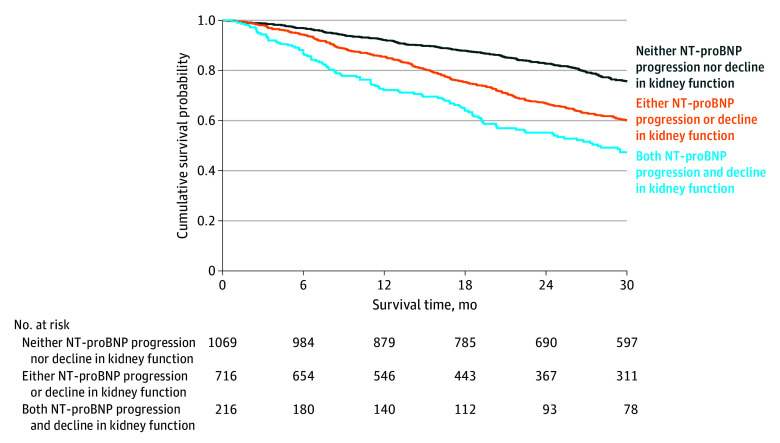
Results: Among 2001 patients, mean (SD) age was 75.5 (8.4) years, and 263 patients (13.1%) were female. The median (IQR) change in eGFR was -5 mlL/min/1.73 m2 (-12 to 1), and 481 patients (24.0%) experienced decline in kidney function. Patients who experienced decline in kidney function more often had the p.(V142I) genotype than patients with stable kidney function (99 [20.6%] vs 202 [13.3%]; P < .001) and had a more severe cardiac phenotype at baseline, as evidenced by higher median (IQR) concentrations of serum cardiac biomarkers (N-terminal pro-B-type natriuretic peptide [NT-proBNP]: 2949 pg/mL [1759-5182] vs 2309 pg/mL [1146-4290]; P < .001; troponin T: 0.060 ng/mL [0.042-0.086] vs 0.052 ng/mL [0.033-0.074]; P < .001), while baseline median (IQR) kidney function was similar between the 2 groups (eGFR: 63 mL/min/1.73 m2 [51-77] vs 61 mL/min/1.73 m2 [49-77]; P = .41). Decline in kidney function was associated with a 1.7-fold higher risk of mortality (hazard ratio [HR], 1.71; 95% CI, 1.43-2.04; P < .001), with a similar risk across the 3 genotypes (wild type: HR, 1.64; 95% CI, 1.31-2.04; p.(V142I): HR, 1.70; 95% CI, 1.21-2.39; non-p.(V142I): HR, 1.51; 95% CI, 0.87-2.61) (P for interaction = .93) and the 3 NAC disease stages (stage 1: HR, 1.69; 95% CI, 1.22-2.32; stage 2: HR, 1.69; 95% CI, 1.30-2.18; stage 3: HR, 1.61; 95% CI, 1.11-2.35) (P for interaction = .97). Decline in kidney function remained independently associated with mortality after adjusting for increases in NT-proBNP and outpatient diuretic intensification (HR, 1.48; 95% CI, 1.23-2.76; P < .001).
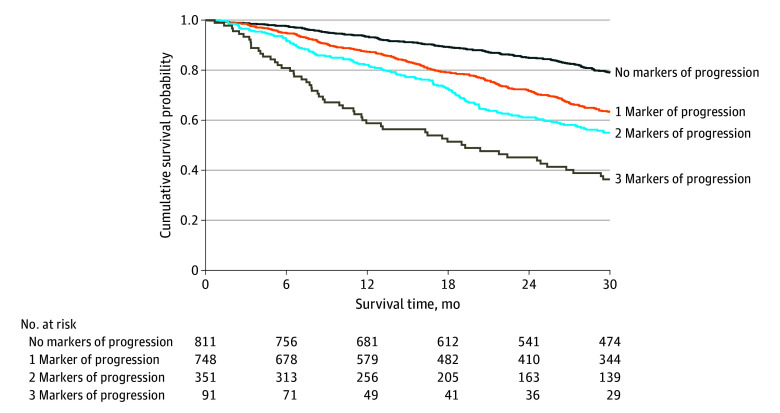
Conclusions and relevance: In this retrospective cohort study, decline in kidney function was frequent in patients with ATTR-CM and was consistently associated with an increased risk of mortality, even after adjusting for established markers of worsening ATTR-CM. eGFR decline represents an independent marker of ATTR-CM disease progression that could guide treatment optimization in clinical practice.
Conflict of interest statement
Figures
References
Publication types
MeSH terms
Substances
Supplementary concepts
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
