

National-level and state-level prevalence of overweight and obesity among children, adolescents, and adults in the USA, 1990-2021, and forecasts up to 2050
- PMID: 39551059
- PMCID: PMC11694015
- DOI: 10.1016/S0140-6736(24)01548-4
National-level and state-level prevalence of overweight and obesity among children, adolescents, and adults in the USA, 1990-2021, and forecasts up to 2050
Abstract
Background: Over the past several decades, the overweight and obesity epidemic in the USA has resulted in a significant health and economic burden. Understanding current trends and future trajectories at both national and state levels is crucial for assessing the success of existing interventions and informing future health policy changes. We estimated the prevalence of overweight and obesity from 1990 to 2021 with forecasts to 2050 for children and adolescents (aged 5-24 years) and adults (aged ≥25 years) at the national level. Additionally, we derived state-specific estimates and projections for older adolescents (aged 15-24 years) and adults for all 50 states and Washington, DC.
Methods: In this analysis, self-reported and measured anthropometric data were extracted from 134 unique sources, which included all major national surveillance survey data. Adjustments were made to correct for self-reporting bias. For individuals older than 18 years, overweight was defined as having a BMI of 25 kg/m2 to less than 30 kg/m2 and obesity was defined as a BMI of 30 kg/m2 or higher, and for individuals younger than 18 years definitions were based on International Obesity Task Force criteria. Historical trends of overweight and obesity prevalence from 1990 to 2021 were estimated using spatiotemporal Gaussian process regression models. A generalised ensemble modelling approach was then used to derive projected estimates up to 2050, assuming continuation of past trends and patterns. All estimates were calculated by age and sex at the national level, with estimates for older adolescents (aged 15-24 years) and adults aged (≥25 years) also calculated for 50 states and Washington, DC. 95% uncertainty intervals (UIs) were derived from the 2·5th and 97·5th percentiles of the posterior distributions of the respective estimates.
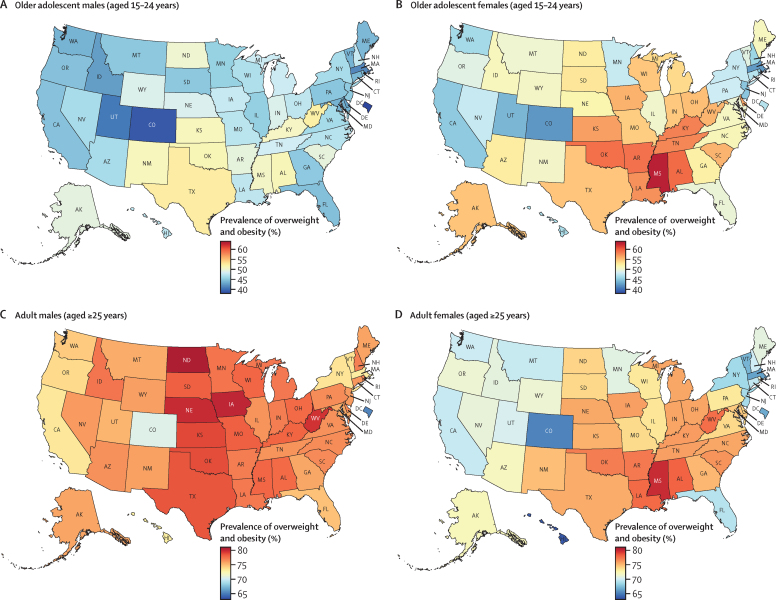
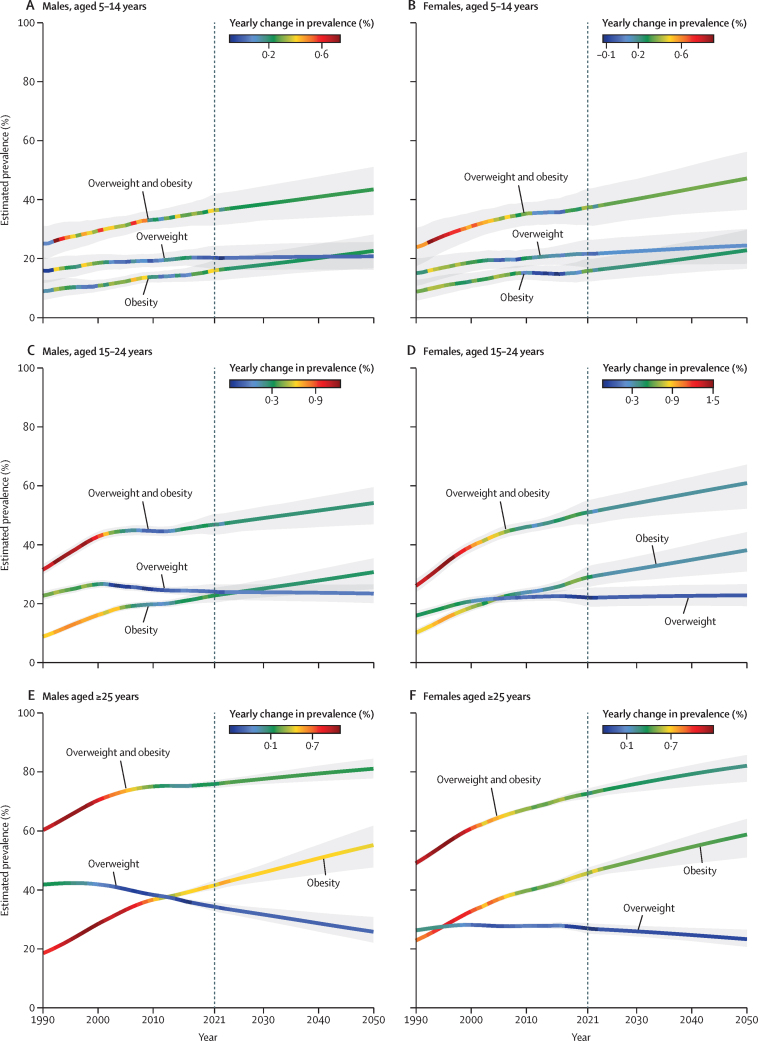
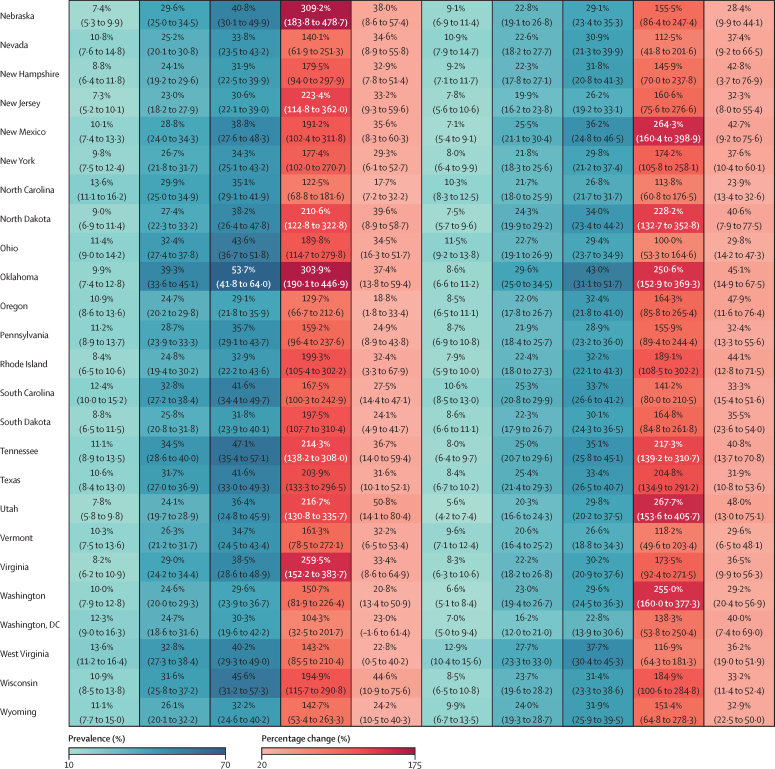
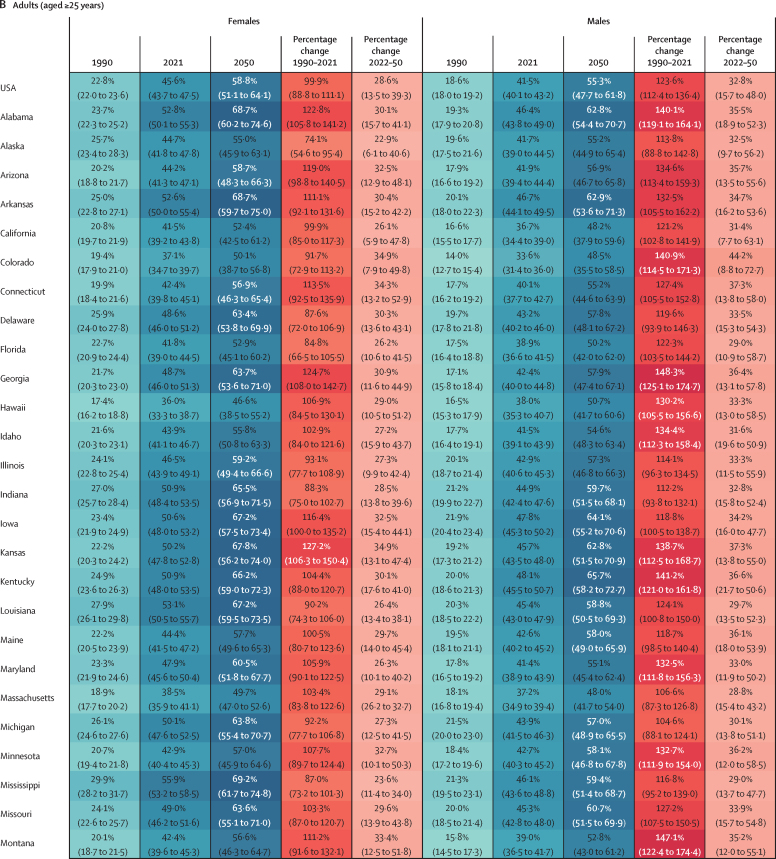
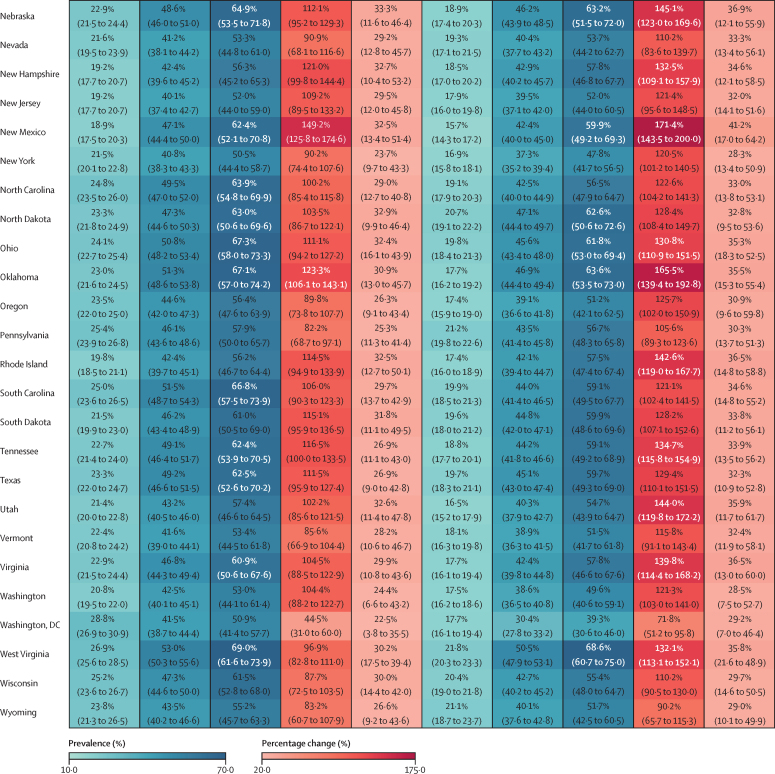
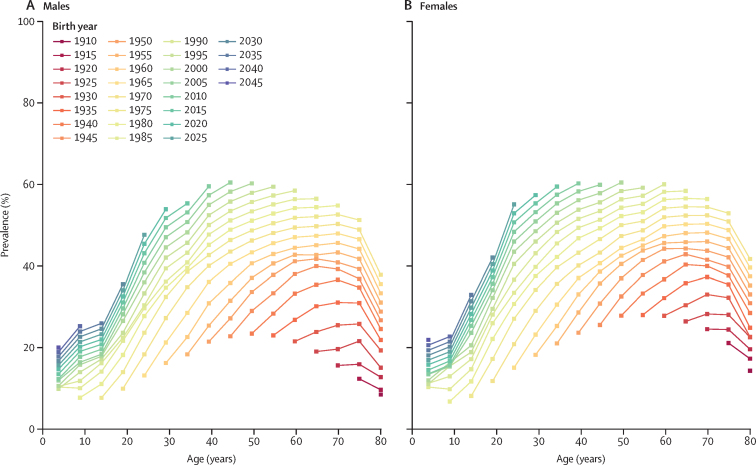
Findings: In 2021, an estimated 15·1 million (95% UI 13·5-16·8) children and young adolescents (aged 5-14 years), 21·4 million (20·2-22·6) older adolescents (aged 15-24 years), and 172 million (169-174) adults (aged ≥25 years) had overweight or obesity in the USA. Texas had the highest age-standardised prevalence of overweight or obesity for male adolescents (aged 15-24 years), at 52·4% (47·4-57·6), whereas Mississippi had the highest for female adolescents (aged 15-24 years), at 63·0% (57·0-68·5). Among adults, the prevalence of overweight or obesity was highest in North Dakota for males, estimated at 80·6% (78·5-82·6), and in Mississippi for females at 79·9% (77·8-81·8). The prevalence of obesity has outpaced the increase in overweight over time, especially among adolescents. Between 1990 and 2021, the percentage change in the age-standardised prevalence of obesity increased by 158·4% (123·9-197·4) among male adolescents and 185·9% (139·4-237·1) among female adolescents (15-24 years). For adults, the percentage change in prevalence of obesity was 123·6% (112·4-136·4) in males and 99·9% (88·8-111·1) in females. Forecast results suggest that if past trends and patterns continue, an additional 3·33 million children and young adolescents (aged 5-14 years), 3·41 million older adolescents (aged 15-24 years), and 41·4 million adults (aged ≥25 years) will have overweight or obesity by 2050. By 2050, the total number of children and adolescents with overweight and obesity will reach 43·1 million (37·2-47·4) and the total number of adults with overweight and obesity will reach 213 million (202-221). In 2050, in most states, a projected one in three adolescents (aged 15-24 years) and two in three adults (≥25 years) will have obesity. Although southern states, such as Oklahoma, Mississippi, Alabama, Arkansas, West Virginia, and Kentucky, are forecast to continue to have a high prevalence of obesity, the highest percentage changes from 2021 are projected in states such as Utah for adolescents and Colorado for adults.
Interpretation: Existing policies have failed to address overweight and obesity. Without major reform, the forecasted trends will be devastating at the individual and population level, and the associated disease burden and economic costs will continue to escalate. Stronger governance is needed to support and implement a multifaceted whole-system approach to disrupt the structural drivers of overweight and obesity at both national and local levels. Although clinical innovations should be leveraged to treat and manage existing obesity equitably, population-level prevention remains central to any intervention strategies, particularly for children and adolescents.
Funding: Bill & Melinda Gates Foundation.
Copyright © 2024 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
Declaration of interests A Al-Ibraheem reports grants or contracts and consulting fees from the International Atomic Energy Agency; participation on a Data Safety Monitoring Board or Advisory Board with the King Hussein Cancer Center; leadership or fiduciary role in other board, society, committee or advocacy group, paid or unpaid, at the World Federation of Nuclear Medicine, Arab Society of Nuclear Medicine, and Jordanian Society of Nuclear Medicine; all outside the submitted work. T W Bärnighausen reports grants or contracts from National Institutes of Health (NIH), Alexander von Humboldt Foundation, German National Research Foundation (DFG), EU, German Ministry of Education and Research, German Ministry of the Environment, Wellcome, and KfW, all through payments to their institution; payment or honoraria for serving as Editor-in-Chief of PLoS Medicine; unpaid participation on Scientific Advisory Boards for two NIH-funded research projects in Africa on Climate Change and Health; stocks in CHEERS, a small-to-medium enterprise focusing on approaches to measure climate change and health-related variables in population cohorts; all outside the submitted work. S Bhaskar reports grants or contracts from Japan Society for the Promotion of Science (JSPS), Japanese Ministry of Education, Culture, Sports, Science and Technology (MEXT) through Grant-in-Aid for Scientific Research (KAKENHI), and from JSPS and the Australian Academy of Science through the JSPS International Fellowship; and leadership or fiduciary role, paid or unpaid, with National Cerebral and Cardiovascular Center (Suita, Osaka, Japan), Rotary District 9675 (Sydney, NSW, Australia), Global Health & Migration Hub Community, Global Health Hub Germany (Berlin, Germany), PLOS One, BMC Neurology, Frontiers in Neurology, Frontiers in Stroke, Frontiers in Aging, Frontiers in Public Health, and BMC Medical Research Methodology, College of Reviewers, Canadian Institutes of Health Research (CIHR), Government of Canada, Cardiff University Biobank (Cardiff, UK), and Cariplo Foundation (Milan, Italy); all outside the submitted work. E J Boyko reports payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing, or educational events from the Korean Diabetes Association, Diabetes Association of the ROC (Taiwan), American Diabetes Association, and International Society for the Diabetic Foot, all outside the submitted work. A Guha reports grants or contracts from the American Heart Association and the US Department of Defense; consulting fees from Pfizer and Novartis; and a leadership or fiduciary role in other board, society, committee or advocacy group, paid or unpaid, with the ZERO Prostate Cancer Health Equity task force; all outside the submitted work. M S Khan reports consulting fees from Bayer outside the submitted work. M Lee reports support for their participation in the present manuscript from the Ministry of Education of the Republic of Korea and the National Research Foundation of Korea (NRF-2023S1A3A2A05095298). S A Meo reports grants or contracts from the Deputyship for Research and Innovation, Ministry of Education in Saudi Arabia (IFKSUOR3-4-10) outside the submitted work. N Scarmeas reports grants or contracts from Novo Nordisk through funding to their institution; participation on a Data Safety Monitoring Board or Advisory Board with the Multicultural Healthy Diet to Reduce Cognitive Decline & AD Risk Safety Monitoring Board and with Primus AD Data Safety Monitoring Board; all outside the submitted work. J A Singh reports consulting fees from ROMTech, Atheneum, Clearview healthcare partners, American College of Rheumatology, Yale, Hulio, Horizon Pharmaceuticals, DINORA, ANI/Exeltis, USA, Frictionless Solutions, Schipher, Crealta/Horizon, Medisys, Fidia, PK Med, Two labs, Adept Field Solutions, Clinical Care options, Putnam associates, Focus forward, Navigant consulting, Spherix, MedIQ, Jupiter Life Science, UBM, Trio Health, Medscape, WebMD, and Practice Point communications and the NIH; payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing or educational events from the speakers bureau of Simply Speaking; support for attending meetings from OMERACT; participation on a Data Safety Monitoring Board or Advisory Board with the US Food and Drug Administration (FDA) Arthritis Advisory Committee; leadership or fiduciary role in other board, society, committee or advocacy group, paid, as a past steering committee member of the OMERACT, and unpaid as Chair of the Veterans Affairs Rheumatology Field Advisory Committee and as the Editor and Director of the UAB Cochrane Musculoskeletal Group Satellite Center on Network Meta-analysis; stock or stock options in Atai life sciences, Kintara Therapeutics, Intelligent Biosolutions, Acumen Pharmaceutical, TPT Global Tech, Vaxart Pharmaceuticals, Atyu Biopharma, Adaptimmune Therapeutics, GeoVax Labs, Pieris Pharmaceuticals, Enzolytics, Seres Therapeutics, Tonix Pharmaceuticals Holding, Aebona Pharmaceuticals, and Charlotte's Web Holdings; and previously owned stock options in Amarin, Viking, and Moderna Pharmaceuticals; all outside the submitted work. D Trico reports payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing or educational events from AstraZeneca, Eli Lilly, and Novo Nordisk; support for attending meetings or travel from AstraZeneca, Eli Lilly, and Novo Nordisk; participation on a Data Safety Monitoring Board or Advisory Board with Amarin; and receipt of equipment, materials, drugs, medical writing, gifts or other services through their institution from PharmaNutra and Abbott; all outside the submitted work. M Zielińska reports other financial or non-financial interests in AstraZeneca as an employee, outside the submitted work.
Figures

Comment in
-
The obesity crisis in the USA: why are there no signs of plateauing yet?Lancet. 2024 Dec 7;404(10469):2241-2242. doi: 10.1016/S0140-6736(24)02467-X. Epub 2024 Nov 14. Lancet. 2024. PMID: 39551060 No abstract available.
References
-
- GBD 2021 Demographics Collaborators Global age-sex-specific mortality, life expectancy, and population estimates in 204 countries and territories and 811 subnational locations, 1950–2021, and the impact of the COVID-19 pandemic: a comprehensive demographic analysis for the Global Burden of Disease Study 2021. Lancet. 2024;403:1989–2056. - PMC - PubMed
-
- GBD 2021 US Burden of Disease Collaborators. The burden of diseases, injuries, and risk factors by state in the USA, 1990–2021: a systematic analysis for the Global Burden of Disease Study 2021. Lancet (in press). - PubMed
-
- Swinburn BA, Kraak VI, Allender S, et al. The global syndemic of obesity, undernutrition, and climate change: The Lancet Commission report. Lancet. 2019;393:791–846. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
