

Effects of tirzepatide on circulatory overload and end-organ damage in heart failure with preserved ejection fraction and obesity: a secondary analysis of the SUMMIT trial
- PMID: 39551891
- PMCID: PMC11835708
- DOI: 10.1038/s41591-024-03374-z
Effects of tirzepatide on circulatory overload and end-organ damage in heart failure with preserved ejection fraction and obesity: a secondary analysis of the SUMMIT trial
Abstract
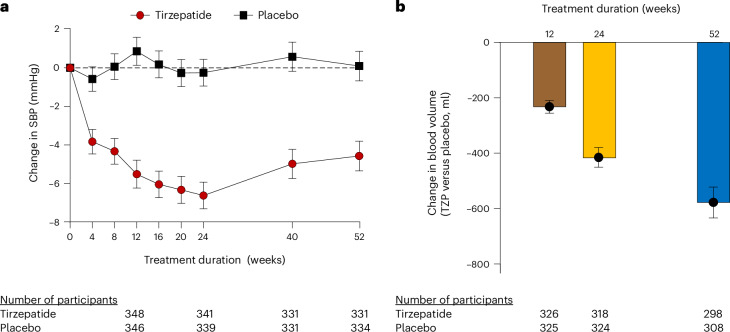
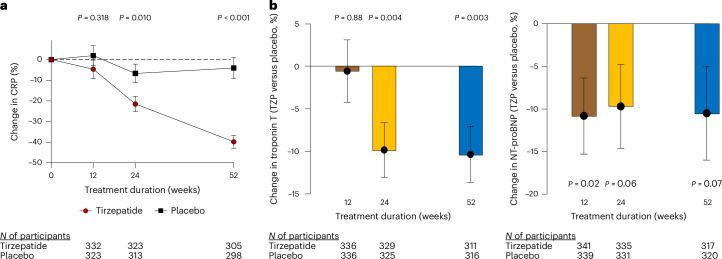
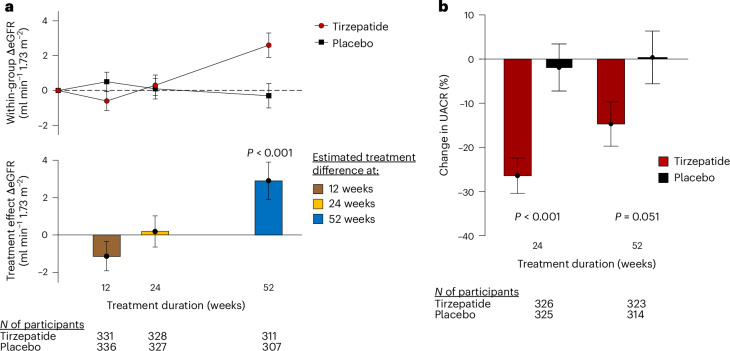
Patients with obesity-related heart failure with preserved ejection fraction (HFpEF) display circulatory volume expansion and pressure overload contributing to cardiovascular-kidney end-organ damage. In the SUMMIT trial, patients with HFpEF and obesity were randomized to the long-acting glucose-dependent insulinotropic polypeptide receptor and glucagon-like peptide-1 receptor agonist tirzepatide (n = 364, 200 women) or placebo (n = 367, 193 women). As reported separately, tirzepatide decreased cardiovascular death or worsening heart failure. Here, in this mechanistic secondary analysis of the SUMMIT trial, tirzepatide treatment at 52 weeks, as compared with placebo, reduced systolic blood pressure (estimated treatment difference (ETD) -5 mmHg, 95% confidence interval (CI) -7 to -3; P < 0.001), decreased estimated blood volume (ETD -0.58 l, 95% CI -0.63 to -0.52; P < 0.001) and reduced C-reactive protein levels (ETD -37.2%, 95% CI -45.7 to -27.3; P < 0.001). These changes were coupled with an increase in estimated glomerular filtration rate (ETD 2.90 ml min-1 1.73 m-2 yr-1, 95% CI 0.94 to 4.86; P = 0.004), a decrease in urine albumin-creatinine ratio (ETD 24 weeks, -25.0%, 95% CI -36 to -13%; P < 0.001; 52 weeks, -15%, 95% CI -28 to 0.1; P = 0.051), a reduction in N-terminal prohormone B-type natriuretic peptide levels (ETD 52 weeks -10.5%, 95% CI -20.7 to 1.0%; P = 0.07) and a reduction in troponin T levels (ETD 52 weeks -10.4%, 95% CI -16.7 to -3.6; P = 0.003). In post hoc exploratory analyses, decreased estimated blood volume with tirzepatide treatment was significantly correlated with decreased blood pressure, reduced microalbuminuria, improved Kansas City Cardiomyopathy Questionnaire Clinical Summary Score and increased 6-min walk distance. Moreover, decreased C-reactive protein levels were correlated with reduced troponin T levels and improved 6-min walk distance. In conclusion, tirzepatide reduced circulatory volume-pressure overload and systemic inflammation and mitigated cardiovascular-kidney end-organ injury in patients with HFpEF and obesity, providing new insights into the mechanisms of benefit from tirzepatide. ClinicalTrials.gov registration: NCT04847557 .
© 2024. The Author(s).
Conflict of interest statement
Competing interests: B.A.B. receives research support from the National Institutes of Health (NIH) and the US Department of Defense, as well as research grant funding from AstraZeneca, Axon, Corvia, Novo Nordisk and Tenax Therapeutics. B.A.B. has served as a consultant for Actelion, Amgen, Aria, Axon Therapies, BD, Boehringer Ingelheim, Cytokinetics, Edwards Lifesciences, Lilly, Imbria, Janssen, Merck, Novo Nordisk, NGM, NXT and VADovations and is named inventor (US patent no. 10,307,179) for the tools and approach for a minimally invasive pericardial modification procedure to treat HF. M.R.Z. receives research support from the Department of Veterans Affairs and serves as a consultant for Abbott, Adona Medical, Aria CV, Avery Therapeutics, Inc., Boehringer Ingelheim, Boston Scientific, Cardiovascular Research Foundation (CRF) Clinical Trials Center, CVRx, DIASTOL Therapeutics, LLC, EBR, Edwards, Lilly, GenKardia, Innoventric, Kestra Medical, Medtronic, Merck, Morphic Therapeutics, Novartis, Pulnovo, Salubris Biotherapeutics, Sonata, sRNAlytics Inc., V-WAVE and Vectorious. C.M.K. has served as a consultant for Eli Lilly. S.J.B. has served as consultant for Altimmune, Amgen, Beren Therapeutics, Boehringer Ingelheim, Lilly, Esperion, Ionis Pharmaceuticals, Madrigal Pharmaceuticals, Merck, Novartis and Regeneron. S.E.L. reported being on the patient selection committee for Corvia and Axon and being a consultant for Novo Nordisk and Lilly. K.H., M.M., Y.O. and N.U. are employed by Eli Lilly and Company. M.P. has served as a consultant for 89bio, AbbVie, Actavis, Altimmune, Alnylam, Amarin, Amgen, Ardelyx, ARMGO, AstraZeneca, Attralus, Biopeutics, Boehringer Ingelheim, Caladrius, Casana, CSL Behring, Cytokinetics, Lilly, Imara, Medtronic, Moderna, Novartis, Pharmacocosmos, Reata, Regeneron, Roche and Salamandra.
Figures
References
-
- Redfield, M. M. & Borlaug, B. A. Heart failure with preserved ejection fraction: a review. JAMA329, 827–838 (2023). - PubMed
-
- Borlaug, B. A., Sharma, K., Shah, S. J. & Ho, J. E. Heart failure with preserved ejection fraction: JACC Scientific Statement. J. Am. Coll. Cardiol.81, 1810–1834 (2023). - PubMed
-
- Ndumele, C. E. et al. Cardiovascular–kidney–metabolic health: a presidential advisory from the American Heart Association. Circulation148, 1606–1635 (2023). - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
