

Early-Stage Extranodal NK/T-Cell Lymphoma, Nasal Type: A Role for Elective Nodal Irradiation?
- PMID: 39553398
- PMCID: PMC11565384
- DOI: 10.1016/j.adro.2024.101650
Early-Stage Extranodal NK/T-Cell Lymphoma, Nasal Type: A Role for Elective Nodal Irradiation?
Abstract
Purpose: Extranodal NK/T-cell lymphoma (ENKTCL) is rare in the Western Hemisphere and is commonly treated with combined modality therapy (CMT).
Methods and materials: We retrospectively reviewed 35 patients treated with Ann Arbor stage I/II ENKTCL between 1994 and 2015 at a large academic cancer center in the United States.
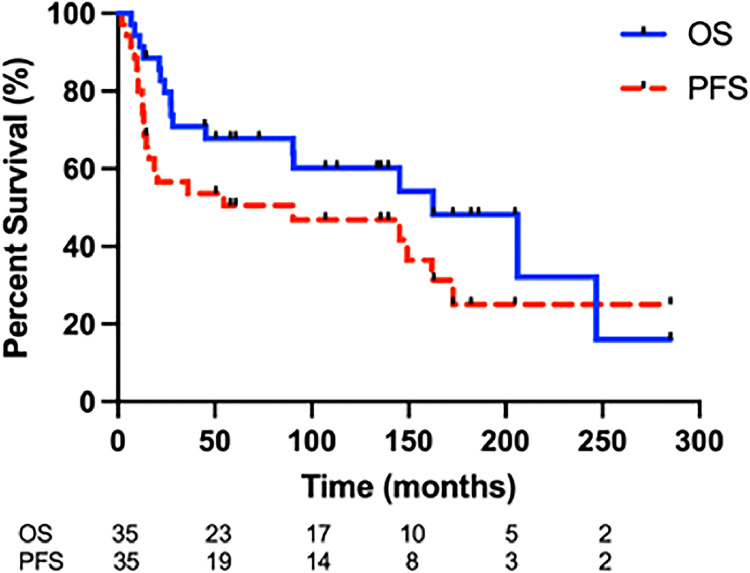
Results: With 11.6 years median follow-up, median overall survival and progression-free survival were 13.5 and 7.5 years, respectively. Eighteen (51%) patients experienced disease relapse, with 5 regional nodal relapses, of which 2 experienced combined regional and distant relapses. All 5 regional nodal relapses occurred exclusively among patients not treated with elective nodal irradiation (ENI). ENI was associated with improved progression-free survival (hazard ratio [HR], 0.21; 95% CI, 0.09-0.52; P = .018) without significant association with OS (HR, 0.33; 95% CI, 0.11-0.94; P = .11). There was a trend toward improved local control with radiation dose to the primary tumor ≥50 Gy (HR, 0.29; 95% CI, 0.08-1.08; P = .098).
Conclusions: In this Western Hemisphere cohort of early-stage ENKTCL patients treated with CMT, ENI may have a potential clinical benefit, particularly in patients who are treated with non-asparaginase-containing CMT, such as in patients treated with radiation alone, patients treated with less intensive chemotherapy concurrently, or patients who are unable to tolerate intensive chemotherapy.
© 2024 The Author(s).
Conflict of interest statement
Paolo Strati is a consultant/on the advisory board for Roche-Genentech, Genmab-AbbVie, Kite-Gilead, Sobi, ADC Therapeutics, and AstraZeneca Acerta and has research support from Kite-Gilead, Sobi, ADC Therapeutics, AstraZeneca Acerta, and ALX Oncology. Loretta J. Nastoupil has received honorariums from AbbVie, AstraZeneca, BMS, Genentech, Genmab, Gilead/Kite, Incyte, Ipsen, Janssen, Merck, Novartis, Regeneron, and Takeda and has received research support from BMS, Caribou Biosciences, Genentech, Genmab, Gilead/Kite, IGM Biosciences, Ipsen, Janssen, Merck, Novartis, and Takeda.
Figures


References
-
- Wang ZY, Liu QF, Wang H, et al. Clinical implications of plasma Epstein-Barr virus DNA in early-stage extranodal nasal-type NK/T-cell lymphoma patients receiving primary radiotherapy. Blood. 2012;120:2003–2010. - PubMed
-
- Yamaguchi M, Suzuki R, Oguchi M. Advances in the treatment of extranodal NK/T-cell lymphoma, nasal type. Blood. 2018;131:2528–2540. - PubMed
-
- Yamaguchi M, Kita K, Miwa H, et al. Frequent expression of P-glycoprotein/MDR1 by nasal T-cell lymphoma cells. Cancer. 1995;76:2351–2356. - PubMed
LinkOut - more resources
Full Text Sources
