

Impact of time to antibiotics on clinical outcome in paediatric febrile neutropenia: a target trial emulation of 1685 episodes
- PMID: 39553416
- PMCID: PMC11566883
- DOI: 10.1016/j.lanwpc.2024.101226
Impact of time to antibiotics on clinical outcome in paediatric febrile neutropenia: a target trial emulation of 1685 episodes
Abstract
Background: Prompt antibiotic administration for febrile neutropenia (FN) is standard of care, and targets of time to antibiotics (TTA) <60 min are common. We sought to determine the effect of TTA ≥60 versus <60 min on adverse outcomes (intensive care unit (ICU) admission or death) in children with cancer and FN. Effect modification by a decision rule that predicts infection (AUS-rule) and bacteraemia were also investigated.
Methods: The prospective, multi-centre (n = 8), Australian PICNICC study dataset was analysed. To control for confounding, we used outcome regression adjusted for propensity score modelled as restricted cubic spline with two degrees of freedom. The propensity score was estimated from a logistic regression model for the exposure on the confounders, identified a priori (age, sex, severely unwell, disease, chemotherapy intensity and site). TTA was defined as time from from emergency triage to first antibiotic dose.
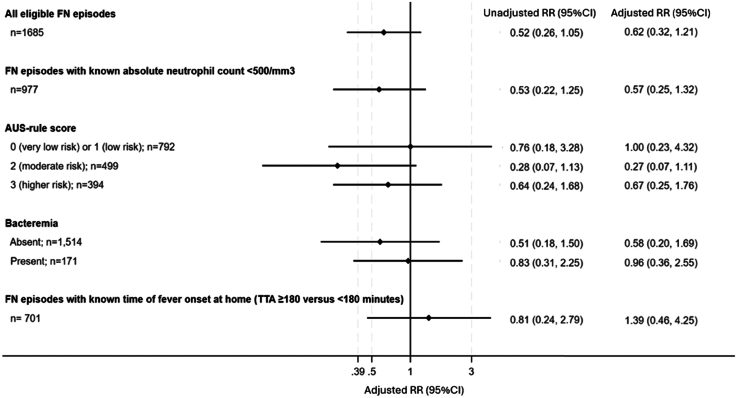
Findings: 1685 FN episodes in 976 patients were included. Median TTA was 53 min (IQR 37-77 min, 1542 (92%) <120 min). An adverse outcome occurred in 43 (2.6%) episodes (39 ICU; 5 deaths). The confounder-adjusted point estimate suggested a lower risk for adverse outcome associated with TTA ≥60 min (RR 0.62, 95% CI 0.32-1.21), but the wide 95% CI precluded definitive judgement about strength and direction of the effect (unadjusted RR 0.52; 95% CI 0.26, 1.05). Similarly, although the point estimates were suggestive of a null association or reduced risk for adverse outcome associated with TTA ≥60 min for all comparisons across bacteraemia or AUS-rule strata, the 95% CIs were imprecise.
Interpretation: For children with FN, there was no definite evidence that TTA ≥60 min from hospital triage (but within 2 h), increased risk of adverse outcome or prolonged hospital admission. This study has important implications for FN TTA mandates, suggesting a more nuanced approach is required.
Funding: National Health and Medical Research Council and Medical Research Future Fund.
Keywords: Children with cancer; Febrile neutropenia (FN); Time to antibiotics (TTA).
© 2024 The Author(s).
Conflict of interest statement
There are no conflicts of interest to disclose.
Figures
References
-
- Lehrnbecher T., Averbuch D., Castagnola E., et al. 8th European Conference on Infections in Leukaemia: 2020 guidelines for the use of antibiotics in paediatric patients with cancer or post-haematopoietic cell transplantation. Lancet Oncol. 2021;22(6):e270–e280. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
