

This is a preprint.
Stratified analysis identifies HIF-2 α as a therapeutic target for highly immune-infiltrated melanomas
- PMID: 39554029
- PMCID: PMC11565796
- DOI: 10.1101/2024.10.29.620300
Stratified analysis identifies HIF-2 α as a therapeutic target for highly immune-infiltrated melanomas
Abstract
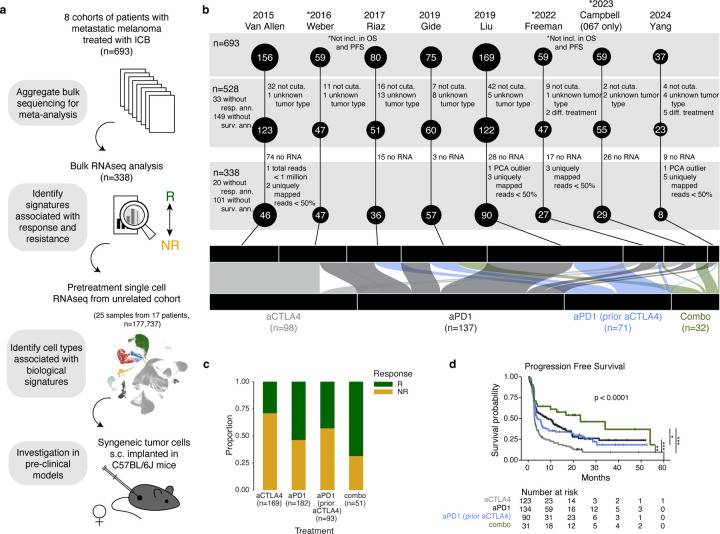
While immune-checkpoint blockade (ICB) has revolutionized treatment of metastatic melanoma over the last decade, the identification of broadly applicable robust biomarkers has been challenging, driven in large part by the heterogeneity of ICB regimens and patient and tumor characteristics. To disentangle these features, we performed a standardized meta-analysis of eight cohorts of patients treated with anti-PD-1 (n=290), anti-CTLA-4 (n=175), and combination anti-PD-1/anti-CTLA-4 (n=51) with RNA sequencing of pre-treatment tumor and clinical annotations. Stratifying by immune-high vs -low tumors, we found that surprisingly, high immune infiltrate was a biomarker for response to combination ICB, but not anti-PD-1 alone. Additionally, hypoxia-related signatures were associated with non-response to anti-PD-1, but only amongst immune infiltrate-high melanomas. In a cohort of scRNA-seq of patients with metastatic melanoma, hypoxia also correlated with immunosuppression and changes in tumor-stromal communication in the tumor microenvironment (TME). Clinically actionable targets of hypoxia signaling were also uniquely expressed across different cell types. We focused on one such target, HIF-2α, which was specifically upregulated in endothelial cells and fibroblasts but not in immune cells or tumor cells. HIF-2α inhibition, in combination with anti-PD-1, enhanced tumor growth control in pre-clinical models, but only in a more immune-infiltrated melanoma model. Our work demonstrates how careful stratification by clinical and molecular characteristics can be leveraged to derive meaningful biological insights and lead to the rational discovery of novel clinical targets for combination therapy.
Keywords: HIF-2α; anti-PD-1; hypoxia; immunotherapy; melanoma.
Conflict of interest statement
Conflict of interest/Competing interest A.H.S. has patents/pending royalties on the PD-1 pathway from Roche and Novartis and has research funding from AbbVie, TaiwanBio, and Calico unrelated to the submitted work. A.H.S. serves on advisory boards for Elpiscience, Monopteros, Alixia, Corner Therapeutics, Bioentre, Amgen, Glaxo Smith Kline, and Janssen. She also is on scientific advisory boards for the Massachusetts General Cancer Center, Program in Cellular and Molecular Medicine at Boston Children’s Hospital, the Human Oncology and Pathogenesis Program at Memorial Sloan Kettering Cancer Center, Perlmutter Cancer Center at NYU, the Gladstone Institutes, and the John Hopkins Bloomberg-Kimmel Institute for Cancer Immunotherapy. She is an academic editor for the Journal of Experimental Medicine. G.J.F. has patents/royalties on the PD-L1/PD-1 pathway from Roche, Merck MSD, Bristol-Myers-Squibb, Merck KGA, Boehringer-Ingelheim, AstraZeneca, Dako, Leica, Mayo Clinic, Eli Lilly, and Novartis. G.J.F. has served on advisory boards for iTeos, NextPoint, IgM, GV20, IOME, Bioentre, Santa Ana Bio, Simcere of America, and Geode. G.J.F. has equity in Nextpoint, iTeos, IgM, Invaria, GV20, Bioentre, and Geode. G.M.B. discloses the following financial and professional collaborations: Takeda Oncology – sponsored research agreement, Olink Proteomics – sponsored research agreement, Novartis – scientific advisory board, speaker, Nektar Therapeutics – scientific advisory board, steering committee, Palleon Pharmaceuticals – sponsored research agreement, InterVenn Biosciences – sponsored research agreement, scientific advisory board, Merck – scientific advisory board, consulting, Iovance - scientific advisory board, Ankyra Therapeutics – scientific advisory board, equity. F.S.H. reports grants and personal fees from Bristol-Myers Squibb, personal fees from Merck, grants and personal fees from Novartis, personal fees from Compass Therapeutics, personal fees from Apricity, personal fees from 7 Hills Pharma, personal fees from Bicara, personal fees from Checkpoint Therapeutics, personal fees from Genentech/Roche, personal fees from Bioentre, personal fees from Gossamer, personal fees from Iovance, personal fees from Catalym, personal fees from Immunocore, personal fees from Kairos, personal fees from Rheos, personal fees from Bayer, personal fees from Zumutor, personal fees from Corner Therapeuitcs, personal fees from Puretech, personal fees from Curis, personal fees from Astra Zeneca, personal fees from Pliant, personal fees from Solu Therapeutics, personal fees from Vir Biotechnology, personal fees from 92Bio, outside the submitted work; In addition, F.S.H. has a patent “Methods for Treating MICA-Related Disorders” (#20100111973) with royalties paid, a patent “Tumor antigens and uses thereof” (#7250291) issued, a patent “Angiopoieten-2 Biomarkers Predictive of Anti-immune checkpoint response” (#20170248603) pending, a patent “Compositions and Methods for Identification, Assessment, Prevention, and Treatment of Melanoma using PD-L1 Isoforms” (#20160340407) pending, a patent “Therapeutic peptides ”(#20160046716) pending, a patent “Therapeutic Peptides” (#20140004112) pending, a patent “Therapeutic Peptides” (#20170022275) pending, a patent “Therapeutic Peptides” (#20170008962) pending, a patent “Therapeutic Peptides” (#9402905) issued, a patent “METHODS OF USING PEMBROLIZUMAB AND TREBANANIB” pending, a patent “Vaccine compositions and methods for restoring NKG2D pathway function against cancers” (#10279021) with royalties paid, a patent “antibodies that bind to MHC Class I polypeptide-related sequence”, a patent (#10106611) issued, a patent “ANTI-GALECTIN ANTIBODY BIOMARKERS PREDICTIVE OF ANTI-IMMUNE CHECKPOINT AND ANTI-ANGIOGENESIS RESPONSES” (publication number #20170343552) pending, and a patent “Antibodies against EDIL3 and methods of use thereof” pending. D.L. reports receiving personal fees from Genentech, and served on the Scientific Advisory Board for Oncovalent Therapeutics, outside the current work.
Figures





References
-
- Stephen Hodi F., O’Day Steven J., McDermott David F., Weber Robert W., Sosman Jeffrey A., Haanen John B., Gonzalez Rene, Robert Caroline, Schadendorf Dirk, Hassel Jessica C., Akerley Wallace, Van Den Eertwegh Alfons J.M., Lutzky Jose, Lorigan Paul, Vaubel Julia M., Linette Gerald P., Hogg David, Ottensmeier Christian H., Lebbé Celeste, Peschel Christian, Quirt Ian, Clark Joseph I., Wolchok Jedd D., Weber Jeffrey S., Tian Jason, Yellin Michael J., Nichol Geoffrey M., Hoos Axel, and Urba Walter J.. Improved Survival with Ipilimumab in Patients with Metastatic Melanoma. New England Journal of Medicine, 363(8):711–723, August 2010. - PMC - PubMed
-
- Robert Caroline, Schachter Jacob, Long Georgina V., Arance Ana, Grob Jean Jacques, Mortier Laurent, Daud Adil, Carlino Matteo S., McNeil Catriona, Lotem Michal, Larkin James, Lorigan Paul, Neyns Bart, Blank Christian U., Hamid Omid, Mateus Christine, Shapira-Frommer Ronnie, Kosh Michele, Zhou Honghong, Ibrahim Nageatte, Ebbinghaus Scot, and Ribas Antoni. Pembrolizumab versus Ipilimumab in Advanced Melanoma. New England Journal of Medicine, 372(26):2521–2532, June 2015. - PubMed
-
- Wolchok Jedd D., Chiarion-Sileni Vanna, Gonzalez Rene, Rutkowski Piotr, Grob Jean-Jacques, Lance Cowey C., Lao Christopher D., Wagstaff John, Schadendorf Dirk, Ferrucci Pier F., Smylie Michael, Dummer Reinhard, Hill Andrew, Hogg David, Haanen John, Carlino Matteo S., Bechter Oliver, Maio Michele, Ivan Marquez-Rodas Massimo Guidoboni, McArthur Grant, Lebbé Celeste, Ascierto Paolo A., Long Georgina V., Cebon Jonathan, Sosman Jeffrey, Postow Michael A., Callahan Margaret K., Walker Dana, Rollin Linda, Bhore Rafia, Stephen Hodi F., and Larkin James. Overall Survival with Combined Nivolumab and Ipilimumab in Advanced Melanoma. New England Journal of Medicine, 377(14):1345–1356, October 2017. - PMC - PubMed
-
- Larkin James, Chiarion-Sileni Vanna, Gonzalez Rene, Grob Jean-Jacques, Rutkowski Piotr, Lao Christopher D., Lance Cowey C., Schadendorf Dirk, Wagstaff John, Dummer Reinhard, Ferrucci Pier F., Smylie Michael, Hogg David, Hill Andrew, Márquez-Rodas Ivan, Haanen John, Guidoboni Massimo, Maio Michele, Schöffski Patrick, Carlino Matteo S., Lebbé Céleste, McArthur Grant, Ascierto Paolo A., Daniels Gregory A., Long Georgina V., Bastholt Lars, Rizzo Jasmine I., Balogh Agnes, Moshyk Andriy, Stephen Hodi F., and Wolchok Jedd D.. Five-Year Survival with Combined Nivolumab and Ipilimumab in Advanced Melanoma. New England Journal of Medicine, 381(16):1535–1546, October 2019. - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources