

This is a preprint.
Systemic inflammation and lymphocyte activation precede rheumatoid arthritis
- PMID: 39554042
- PMCID: PMC11565773
- DOI: 10.1101/2024.10.25.620344
Systemic inflammation and lymphocyte activation precede rheumatoid arthritis
Update in
-
Progression to rheumatoid arthritis in at-risk individuals is defined by systemic inflammation and by T and B cell dysregulation.Sci Transl Med. 2025 Sep 24;17(817):eadt7214. doi: 10.1126/scitranslmed.adt7214. Epub 2025 Sep 24. Sci Transl Med. 2025. PMID: 40991726
Abstract
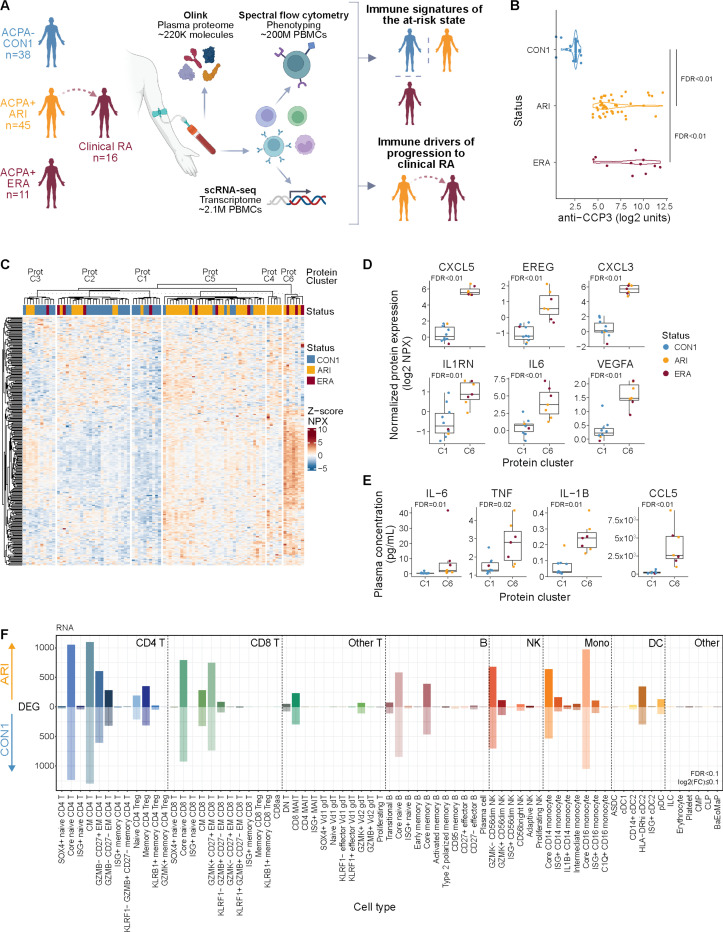
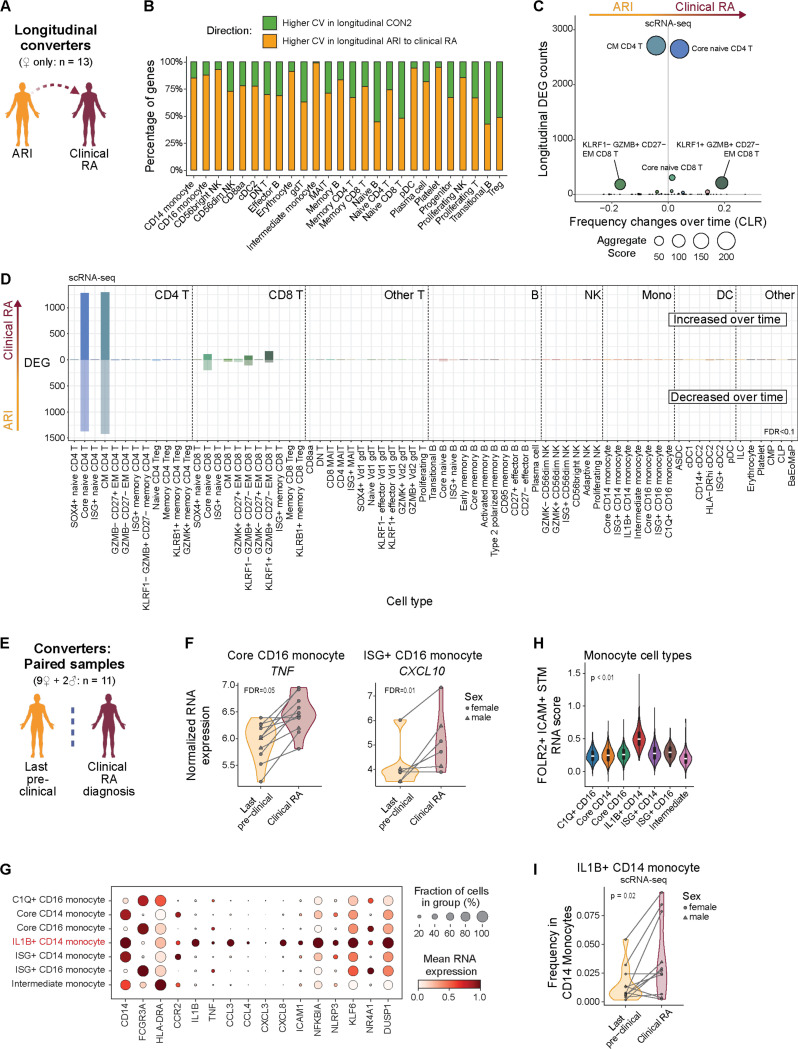
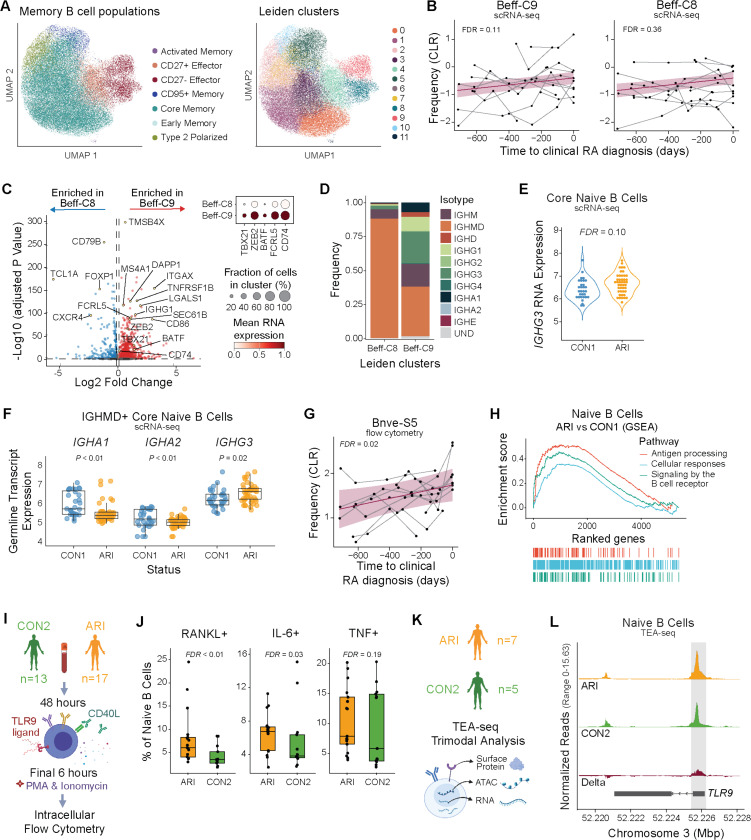
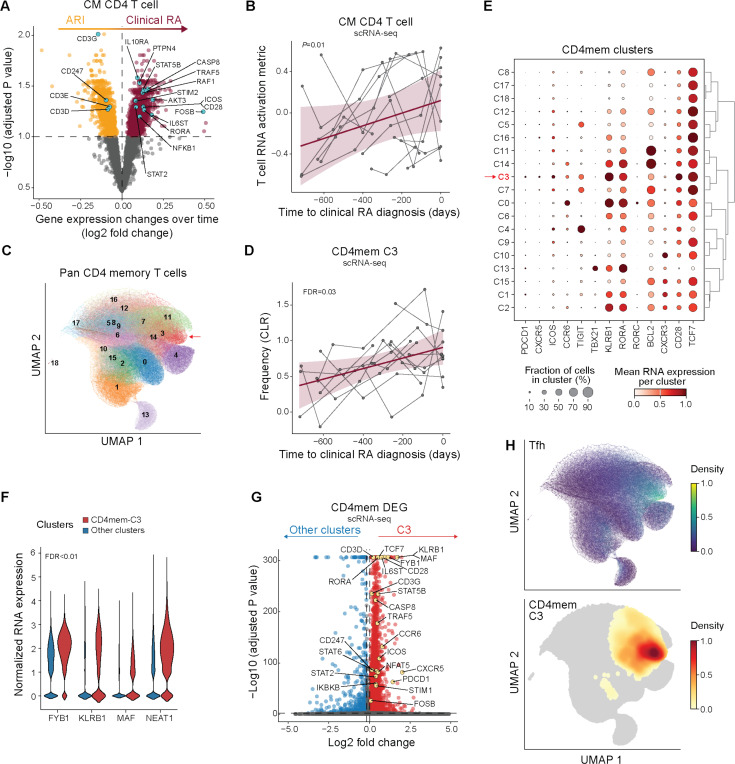
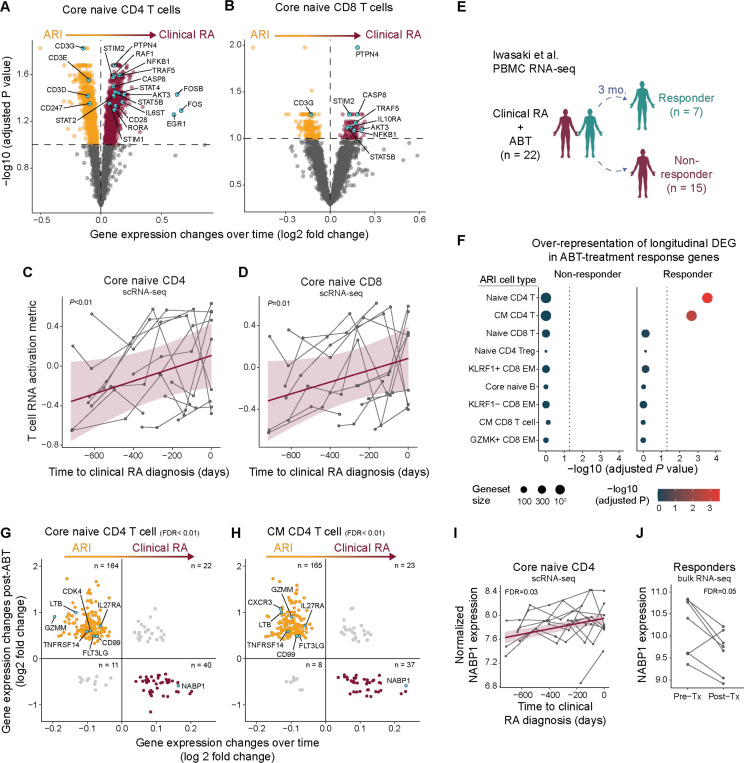
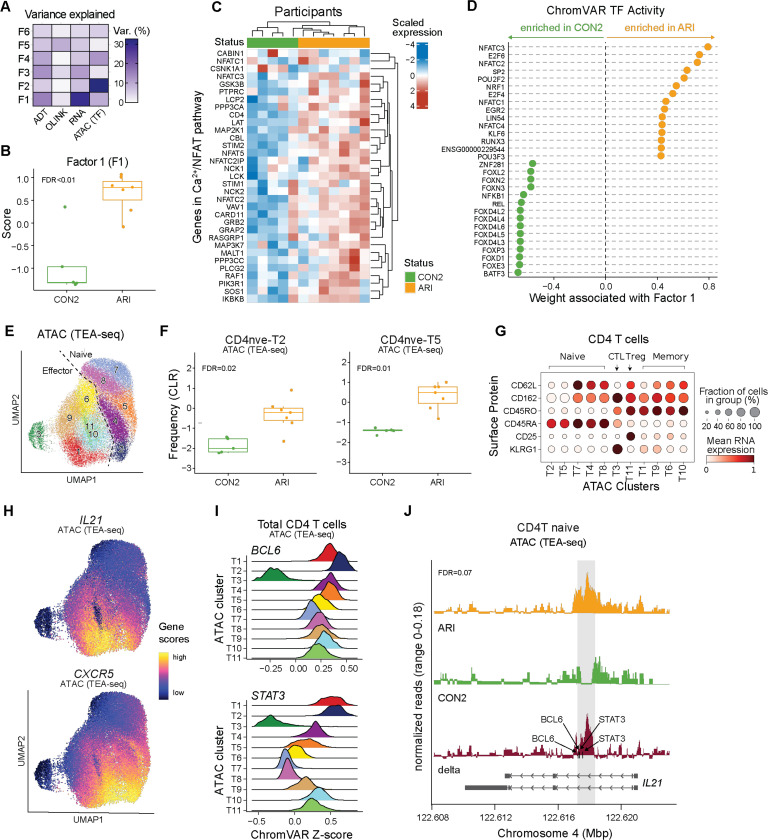
Some autoimmune diseases, including rheumatoid arthritis (RA), are preceded by a critical subclinical phase of disease activity. Proactive clinical management is hampered by a lack of biological understanding of this subclinical 'at-risk' state and the changes underlying disease development. In a cross-sectional and longitudinal multi-omics study of peripheral immunity in the autoantibody-positive at-risk for RA period, we identified systemic inflammation, proinflammatory-skewed B cells, expanded Tfh17-like cells, epigenetic bias in naive T cells, TNF+IL1B+ monocytes resembling a synovial macrophage population, and CD4 T cell transcriptional features resembling those suppressed by abatacept (CTLA4-Ig) in RA patients. Our findings characterize pathogenesis prior to clinical diagnosis and suggest the at-risk state exhibits substantial immune alterations that could potentially be targeted for early intervention to delay or prevent autoimmunity. We provide a suite of tools at https://apps.allenimmunology.org/aifi/insights/ra-progression/ to facilitate exploration and enhance accessibility of this extensive dataset.
Figures
References
-
- Combe B., Landewe R., Daien C. I., Hua C., Aletaha D., Álvaro-Gracia J. M., Bakkers M., Brodin N., Burmester G. R., Codreanu C., Conway R., Dougados M., Emery P., Ferraccioli G., Fonseca J., Raza K., Silva-Fernández L., Smolen J. S., Skingle D., Szekanecz Z., Kvien T. K., van A. der Helm-van Mil, van Vollenhoven R., 2016 update of the EULAR recommendations for the management of early arthritis. Ann. Rheum. Dis. 76, 948–959 (2017). - PubMed
-
- Herold K. C., Bundy B. N., Long S. A., Bluestone J. A., DiMeglio L. A., Dufort M. J., Gitelman S. E., Gottlieb P. A., Krischer J. P., Linsley P. S., Marks J. B., Moore W., Moran A., Rodriguez H., Russell W. E., Schatz D., Skyler J. S., Tsalikian E., Wherrett D. K., Ziegler A.-G., Greenbaum C. J., Type 1 Diabetes TrialNet Study Group, An Anti-CD3 Antibody, Teplizumab, in Relatives at Risk for Type 1 Diabetes. N. Engl. J. Med. 381, 603–613 (2019). - PMC - PubMed
-
- Buch M. H., Defining refractory rheumatoid arthritis. Ann. Rheum. Dis. 77, 966–969 (2018). - PubMed
-
- Rantapää-Dahlqvist S., de Jong B. A. W., Berglin E., Hallmans G., Wadell G., Stenlund H., Sundin U., van Venrooij W. J., Antibodies against cyclic citrullinated peptide and IgA rheumatoid factor predict the development of rheumatoid arthritis. Arthritis Rheum. 48, 2741–2749 (2003). - PubMed
-
- Nielen M. M. J., van Schaardenburg D., Reesink H. W., van de Stadt R. J., van der Horst-Bruinsma I. E., de Koning M. H. M. T., Habibuw M. R., Vandenbroucke J. P., Dijkmans B. A. C., Specific autoantibodies precede the symptoms of rheumatoid arthritis: a study of serial measurements in blood donors. Arthritis Rheum. 50, 380–386 (2004). - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials