

Glial fibrillary acidic protein in Alzheimer's disease: a narrative review
- PMID: 39554381
- PMCID: PMC11568389
- DOI: 10.1093/braincomms/fcae396
Glial fibrillary acidic protein in Alzheimer's disease: a narrative review
Abstract
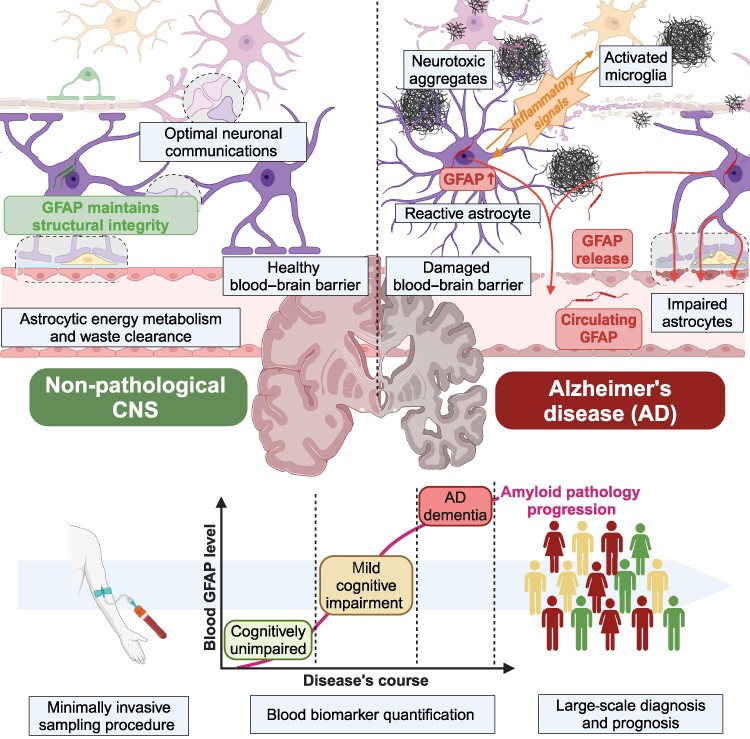
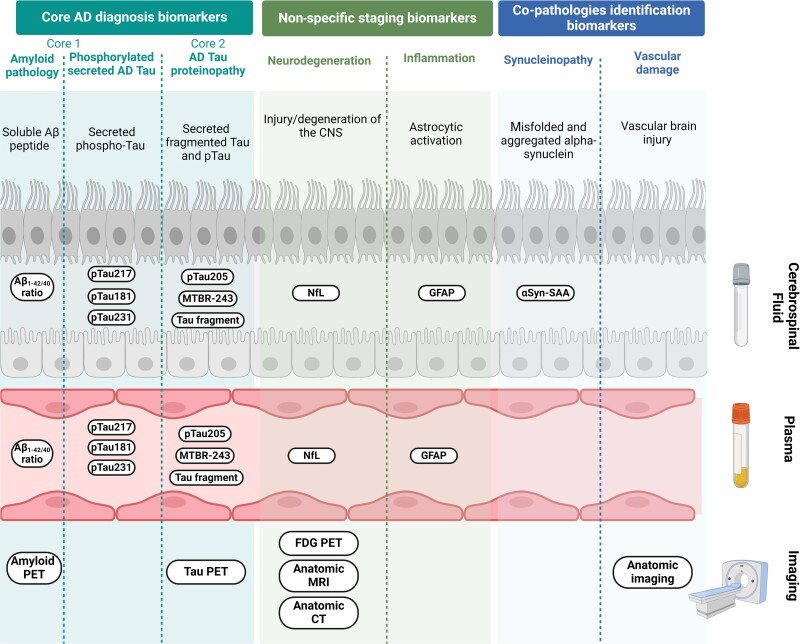
Astrocytes are fundamental in neural functioning and homeostasis in the central nervous system. These cells respond to injuries and pathological conditions through astrogliosis, a reactive process associated with neurodegenerative diseases such as Alzheimer's disease. This process is thought to begin in the early stages of these conditions. Glial fibrillary acidic protein (GFAP), a type III intermediate filament protein predominantly expressed in astrocytes, has emerged as a key biomarker for monitoring this response. During astrogliosis, GFAP is released into biofluids, making it a candidate for non-invasive diagnosis and tracking of neurodegenerative diseases. Growing evidence positions GFAP as a biomarker for Alzheimer's disease with specificity and disease-correlation characteristics comparable to established clinical markers, such as Aβ peptides and phosphorylated tau protein. To improve diagnostic accuracy, particularly in the presence of confounders and comorbidities, incorporating a panel of biomarkers may be advantageous. This review will explore the potential of GFAP within such a panel, examining its role in early diagnosis, disease progression monitoring and its integration into clinical practice for Alzheimer's disease management.
Keywords: Alzheimer’s disease; astrocytes; biomarker; glial fibrillary acidic protein; reactive astrogliosis.
© The Author(s) 2024. Published by Oxford University Press on behalf of the Guarantors of Brain.
Conflict of interest statement
The authors report no competing interests.
Figures

References
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous