

Home-Use and Portable Biofeedback Lowers Anxiety and Pain in Chronic Pain Subjects
- PMID: 39554946
- PMCID: PMC11562280
- DOI: 10.1177/15598276231221112
Home-Use and Portable Biofeedback Lowers Anxiety and Pain in Chronic Pain Subjects
Abstract
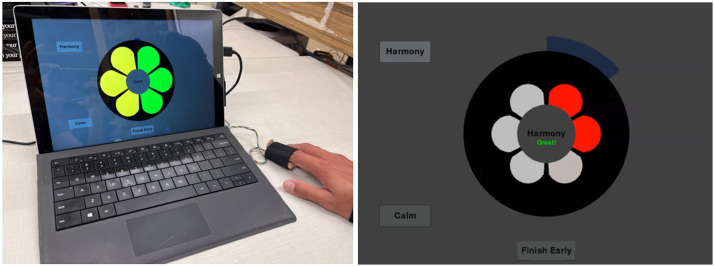
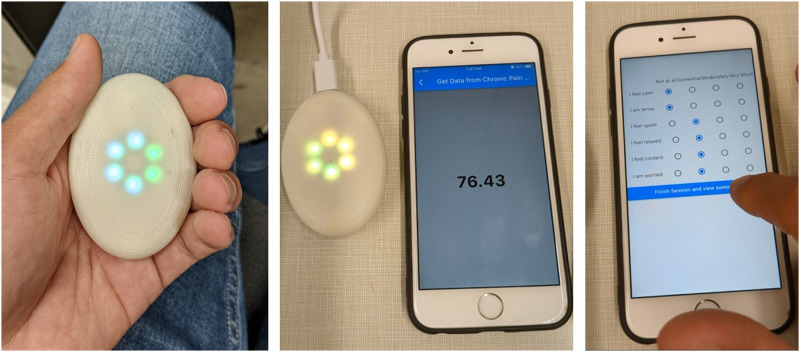
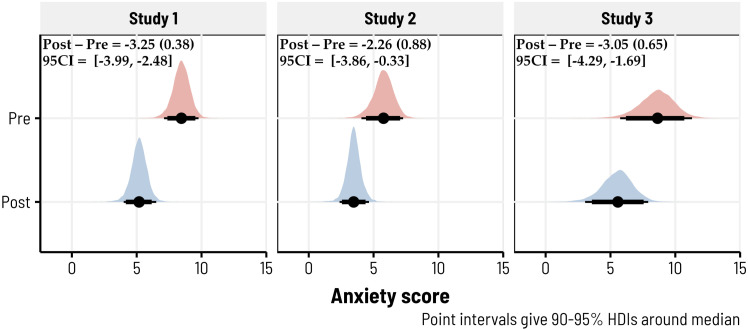
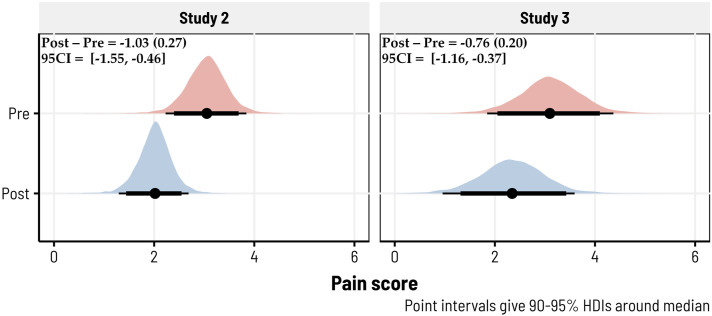
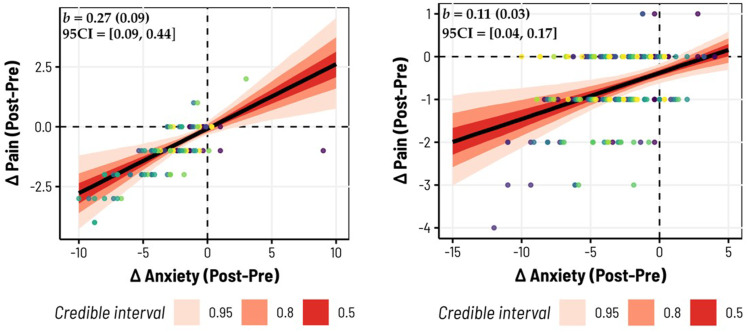
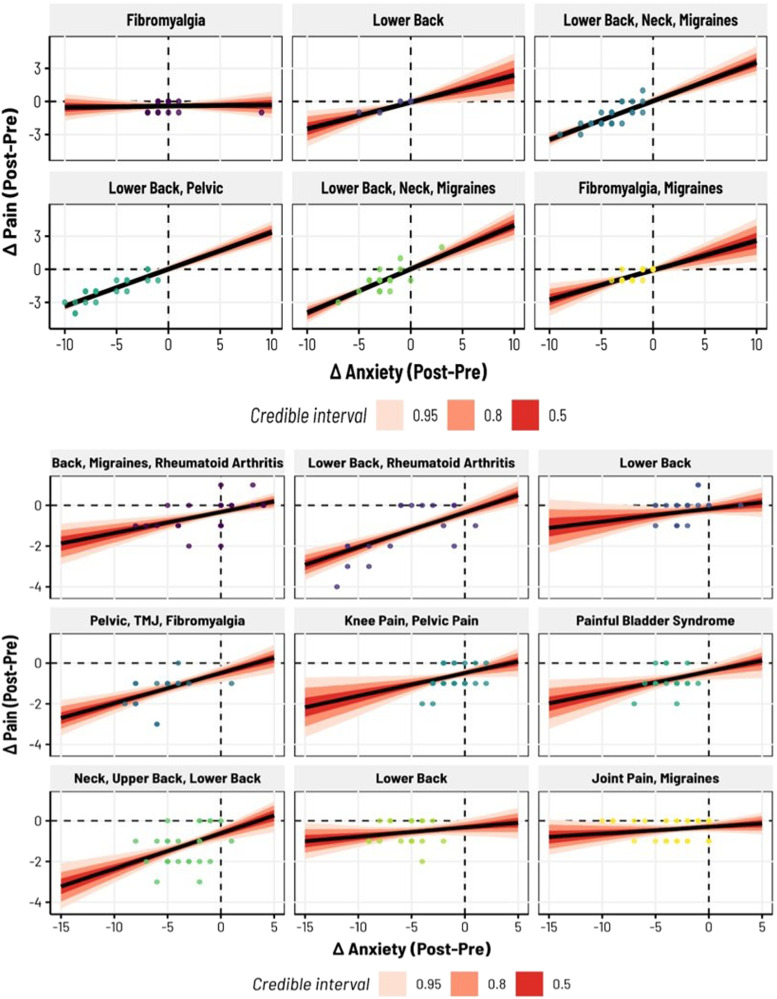
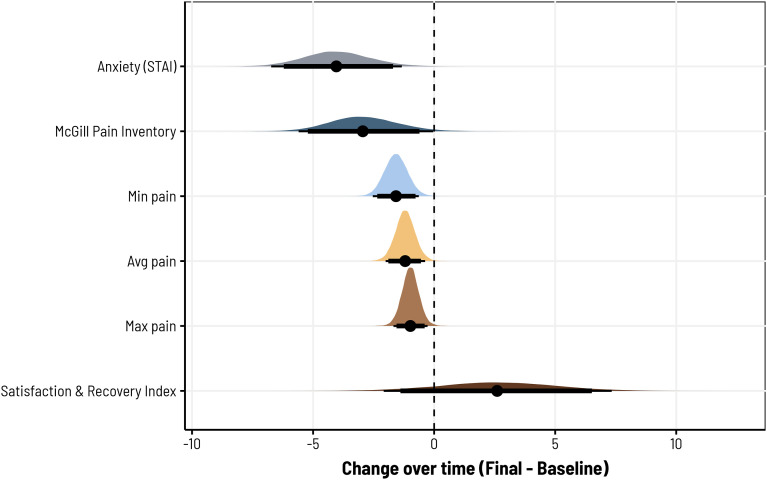
In this study, we investigated the use of novel, home-use and portable biofeedback devices in a remote program for managing chronic pain. In three separate 4-week pilot studies, participants engaged in twice-daily, 10-minute biofeedback sessions, with self-assessed reductions in anxiety and pain levels using the 6-item State-Trait Anxiety Inventory (STAI-6) and Visual Analogue Scale (VAS), respectively, in Studies 2 and 3. Among these 113 (Study 2) and 237 (Study 3) biofeedback sessions, 81 (∼72%) and 130 (∼55%) showed reductions in pain, while 93 (∼82%) and 184 (∼78%) experienced reductions in anxiety. A positive relationship was found between anxiety and pain reduction, indicating that larger reductions in anxiety correspond to larger reductions in pain. In Study 1, only anxiety reductions were measured: across 143 biofeedback sessions, 127 experienced reductions in anxiety (∼89%). Participants in all studies demonstrated reductions in baseline to final results in pain, anxiety, and showed increases in satisfaction and recovery. Our results provide strong evidence that portable biofeedback devices can enhance pain management programs by helping to alleviate anxiety and pain in individuals living with chronic conditions. This study can provide a basis for the integration of biofeedback devices into the expanding research of lifestyle and integrative medicine.
Keywords: anxiety; biofeedback; chronic pain; portable.
Copyright © 2023 The Author(s).
Conflict of interest statement
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures
References
-
- Gatchel RJ, McGeary DD, McGeary CA, Lippe B. Interdisciplinary chronic pain management: past, present, and future. Am Psychol. 2014;69(2):119. - PubMed
-
- Zhao Y, Ly F, Hong Q, et al. How much does it hurt: a deep learning framework for chronic pain score assessment. In: 2020 International Conference on Data Mining Workshops (ICDMW); November 17 2020; Sorrento, Italy:651-660: IEEE.
LinkOut - more resources
Full Text Sources