

Sex-specific dementia risk in known or suspected obstructive sleep apnea: a 10-year longitudinal population-based study
- PMID: 39554998
- PMCID: PMC11568356
- DOI: 10.1093/sleepadvances/zpae077
Sex-specific dementia risk in known or suspected obstructive sleep apnea: a 10-year longitudinal population-based study
Abstract
Study objectives: To evaluate sex-specific associations between known or suspected obstructive sleep apnea (OSA) and dementia risk over 10 years among older women and men.
Methods: This study included 18 815 women and men age 50+ years (dementia-free at baseline) who participated in the Health and Retirement Study (HRS), a nationally representative cohort of US adults. Presence of OSA was defined by self-reported diagnosis or key HRS items that correspond to elements of a validated OSA screening tool (STOP-Bang). Incident dementia cases were identified using a validated, HRS-based algorithm derived from objective cognitive assessments. Survey-weighted regression models based on pseudo-values were utilized to estimate sex- and age-specific differences in cumulative incidence of dementia by OSA status.
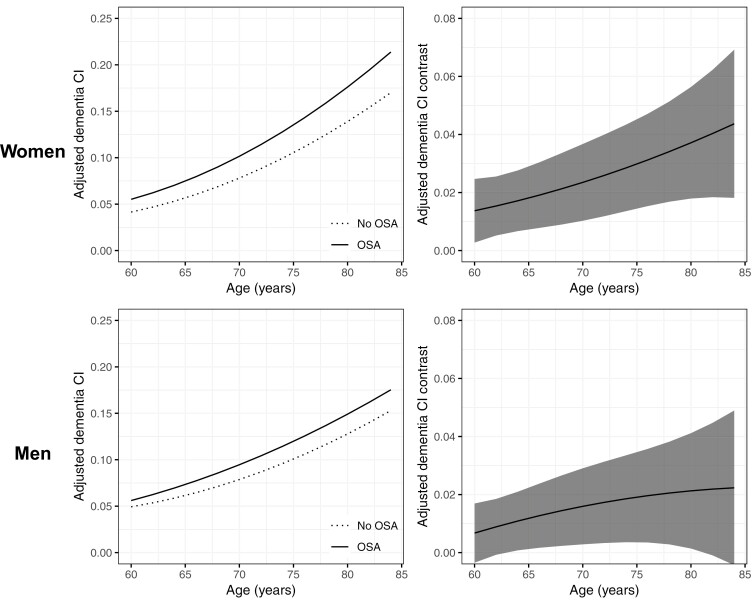
Results: Data from 18 815 adults were analyzed, of which 9% of women and 8% of men (weighted proportions) met criteria for incident dementia. Known/suspected OSA was more prevalent in men than in women (weighted proportions 68% vs. 31%). Unadjusted sex-stratified analyses showed that known/suspected OSA was associated with higher cumulative incidence of dementia across ages 60-84 years for women and men. By age 80, relative to adults without known/suspected OSA, the cumulative incidence of dementia was 4.7% higher (CI 2.8%, 6.7%) for women with known/suspected OSA, and 2.5% (CI 0.5%, 4.5%) for men with known/suspected OSA, respectively. Adjusted associations between age-specific OSA and cumulative incidence of dementia attenuated for both women and men but remained statistically significant.
Conclusions: OSA contributes to dementia risk in older adults, particularly women. This study illuminates the impact of a potentially modifiable yet frequently overlooked risk factor for dementia onset.
Keywords: OSA; cognitive function; dementia; neurodegenerative disorders; neurological disorders; women’s health.
© The Author(s) 2024. Published by Oxford University Press on behalf of Sleep Research Society.
Figures

References
-
- Hudomiet P, Hurd MD, Rohwedder S.. Trends in inequalities in the prevalence of dementia in the United States. Proc Natl Acad Sci U S A. 2022;119(46):e2212205119. doi: https://doi.org/ 10.1073/pnas.2212205119 - DOI - PMC - PubMed
-
- Rajan KB, Weuve J, Barnes LL, McAninch EA, Wilson RS, Evans DA.. Population estimate of people with clinical Alzheimer’s disease and mild cognitive impairment in the United States (2020-2060). Alzheimers Dement. 2021;17(12):1966–1975. doi: https://doi.org/ 10.1002/alz.12362 - DOI - PMC - PubMed
-
- Dilworth-Anderson P, Hendrie HC, Manly JJ, Khachaturian AS, Fazio S; Social, Behavioral and Diversity Research Workgroup of the Alzheimer’s Association. Diagnosis and assessment of Alzheimer’s disease in diverse populations. Alzheimers Dement. 2008;4(4):305–309. doi: https://doi.org/ 10.1016/j.jalz.2008.03.001 - DOI - PubMed
-
- Manly JJ, Mayeux R.. Ethnic Differences in Dementia and Alzheimer’s Disease. In: Anderson NB, Bulatao RA, Cohen B, eds. Critical Perspectives on Racial and Ethnic Differences in Health in Late Life. Washington (DC): National Academies Press; 2004: 95–141. - PubMed
-
- Demirovic J, Prineas R, Loewenstein D, et al. Prevalence of dementia in three ethnic groups: the South Florida program on aging and health. Ann Epidemiol. 2003;13(6):472–478. doi: https://doi.org/ 10.1016/s1047-2797(02)00437-4 - DOI - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
