

Comparison of Clinical Outcomes Between Nonoperative Treatment and Arthroscopically Assisted Stabilization in Patients With Acute Rockwood Type 5 Acromioclavicular Dislocation
- PMID: 39555319
- PMCID: PMC11565689
- DOI: 10.1177/23259671241289117
Comparison of Clinical Outcomes Between Nonoperative Treatment and Arthroscopically Assisted Stabilization in Patients With Acute Rockwood Type 5 Acromioclavicular Dislocation
Abstract
Background: Currently, Rockwood type 3 acromioclavicular (AC) joint dislocations are initially treated nonoperatively, whereas surgery is recommended for Rockwood type 5 dislocations. However, multiple studies have been published favoring nonoperative approaches in patients with high-grade Rockwood injuries.
Purpose: To compare the clinical and radiological outcomes of patients with acute Rockwood type 5 AC joint dislocations treated nonoperatively versus with arthroscopically assisted stabilization.
Study design: Cohort study; Level of evidence, 3.
Methods: Included were 48 patients with acute Rockwood type 5 dislocation who were initially treated nonoperatively between June 2010 and June 2022 and 48 patients matched according to age, sex, affected side, and follow-up interval who underwent arthroscopically assisted coracoclavicular (CC) stabilization using a suture-button technique, with additional percutaneous AC tape cerclage. Clinical outcomes were assessed based on the Subjective Shoulder Value, Nottingham Clavicle Score, Constant score, and visual analog scale for pain. The radiographic assessment included the CC distance, CC difference ratio, and degree of horizontal instability at final follow-up (62 ± 43 months).
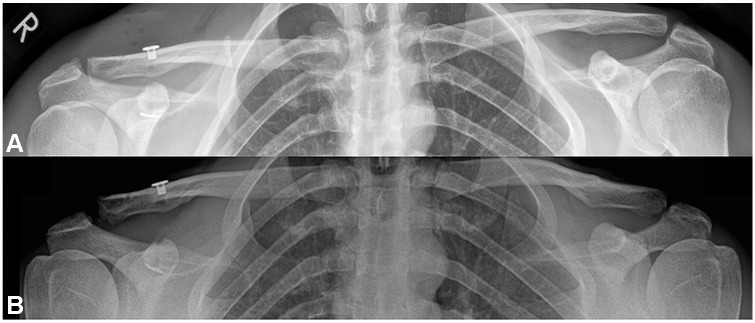
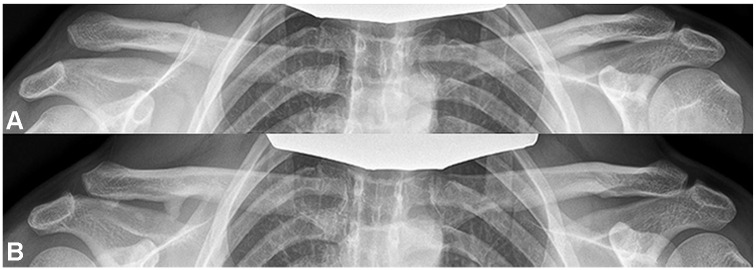
Results: At the final follow-up, the Constant score was significantly higher in the nonoperative group (P = .02). The operative group had significantly higher pain levels on palpation of the AC joint (1.2 ± 2.2 vs 0.19 ± 0.5 for the nonoperative group; P = .003). In the operative group, the mean CC difference ratio was significantly higher at the latest follow-up compared with postoperatively (1.3 ± 0.3 vs 0.67 ± 0.3, respectively; P < .001), whereas the CC difference ratio of the nonoperative group was significantly reduced at the latest follow-up compared with postinjury (2.0 ± 0.5 vs 2.6 ± 0.8, respectively; P < .001). The operative group had a significantly lower CC difference ratio compared with the nonoperative group at final follow-up (P < .001). More than half of the patients (56%) who were treated operatively had a loss of reduction resulting in a Rockwood type 3 state at the latest follow-up, whereas 54% of patients treated nonoperatively had spontaneous reduction of injury severity from Rockwood type 5 to Rockwood type 3.
Conclusion: Although 15% of the nonoperatively treated patients eventually required surgery, successful nonoperative treatment showed similar outcomes to initial operative treatment in patients with acute Rockwood type 5 dislocation.
Keywords: Rockwood type 5; acromioclavicular dislocation; acute; nonoperative treatment; suture-button technique.
© The Author(s) 2024.
Conflict of interest statement
One or more of the authors has declared the following potential conflict of interest or source of funding: D.A. has received consulting fees from Arthrex and Medacta. P.M. has received consulting fees from Alyve Medical, Arthrex, and Medacta. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Figures
References
-
- Alexander OM. Radiography of the acromioclavicular articulation. Med Radiogr Photogr. 1954;30(2):34-39. - PubMed
-
- Balke M, Schneider MM, Shafizadeh S, Bäthis H, Bouillon B, Banerjee M. Current state of treatment of acute acromioclavicular joint injuries in Germany: is there a difference between specialists and non-specialists? A survey of German trauma and orthopaedic departments. Knee Surg Sports Traumatol Arthrosc. 2015;23(5):1447-1452. - PubMed
-
- Barth J, Duparc F, Andrieu K, et al. Is coracoclavicular stabilisation alone sufficient for the endoscopic treatment of severe acromioclavicular joint dislocation (Rockwood types III, IV, and V)? Orthop Traumatol Surg Res. 2015;101(8 suppl):S297-S303. - PubMed
-
- Beitzel K, Cote MP, Apostolakos J, et al. Current concepts in the treatment of acromioclavicular joint dislocations. Arthroscopy. 2013;29(2):387-397. - PubMed
LinkOut - more resources
Full Text Sources
