

Alternative lengthening of telomere-based immortalization renders H3G34R-mutant diffuse hemispheric glioma hypersensitive to PARP inhibitor combination regimens
- PMID: 39556024
- PMCID: PMC11889718
- DOI: 10.1093/neuonc/noae228
Alternative lengthening of telomere-based immortalization renders H3G34R-mutant diffuse hemispheric glioma hypersensitive to PARP inhibitor combination regimens
Abstract
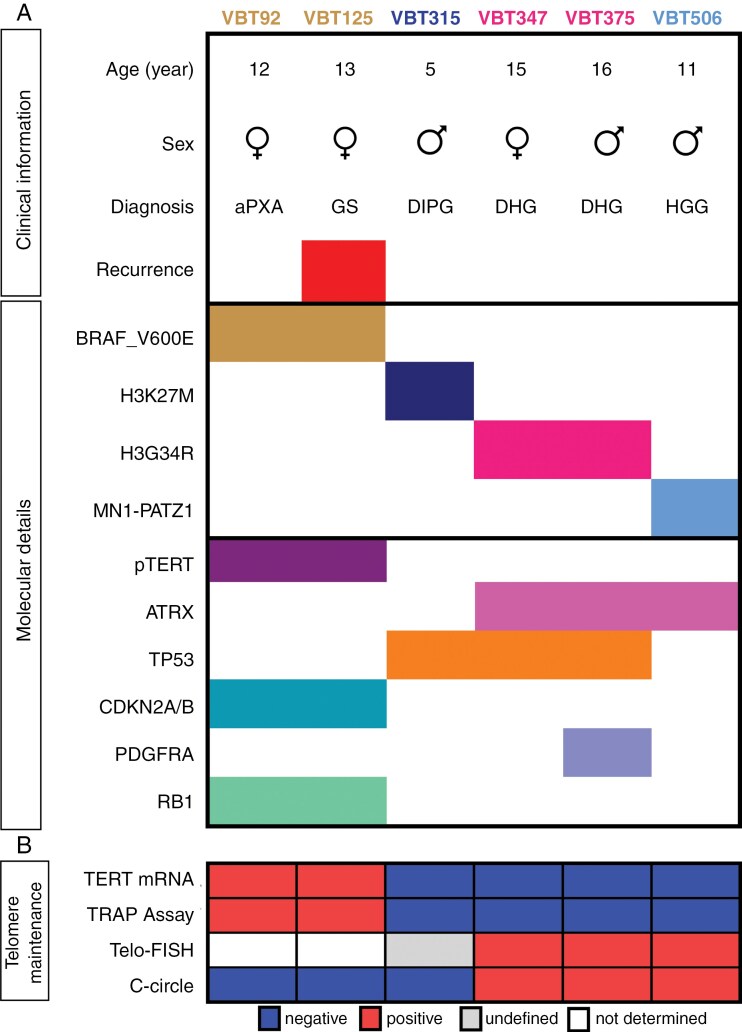
Background: Diffuse hemispheric glioma, H3 G34R/V-mutant (DHG-H3G34) is characterized by poor prognosis and lack of effective treatment options. DHG-H3G34R further harbor deactivation of alpha-thalassemia/mental retardation syndrome X-linked protein (ATRX; DHG-H3G34R_ATRX) suggesting a unique interaction of these 2 oncogenic alterations. In this study, we dissect their cell biological interplay, investigate the impact on telomere stabilization, and consequently validate a targeted therapy approach.
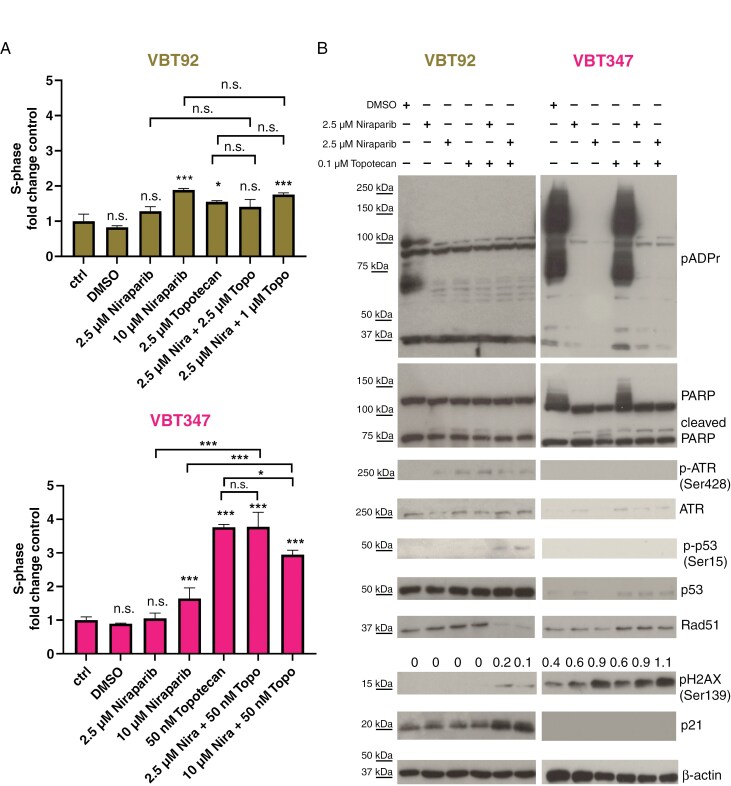
Methods: We characterized patient-derived primary pediatric high-grade glioma (pHGG) models for telomere-maintenance mechanisms, DNA damage stress (including protein expression, pH2AX/Rad51 foci, cell-cycle arrest) and their sensitivity towards poly-ADP ribose polymerase inhibitor (PARPi) combinations. Human induced pluripotent stem cells (iPSCs) were used for modeling the disease. The anticancer activity of PARPi combinations in vivo was studied in Chorioallantoic Membrane (CAM) and orthotopic in vivo experiments. Finally, we treated a DHG-H3G34R_ATRX patient with PARPi combination therapy.
Results: We elaborate that alternative lengthening of telomeres (ALT) is a key characteristic of DHG-H3G34R_ATRX. A dominant cooperative effect between H3G34R and ATRX loss in ALT activation also became apparent in iPSCs, which endogenously exert telomerase activity. In both, patient-derived DHG-H3G34R_ATRX models and H3G34R+/ATRX- iPSCs, the ALT-phenotype was associated with increased basal DNA damage stress, mediating synergistic susceptibility towards PARPi (talazoparib, niraparib) combinations with topoisomerase-I inhibitors (topotecan, irinotecan). In a first-of-its-kind case, treatment of a DHG-H3G34R_ATRX patient with the brain-penetrant PARP inhibitor niraparib and topotecan resulted in significant tumor reduction.
Conclusions: Our preclinical and clinical data strongly support the further development of PARPi together with DNA damage stress-inducing treatment regimens for DHG-H3G34R_ATRX.
Keywords: ATRX; DNA damage; H3G34R; PARP inhibitor; diffuse hemispheric glioma.
© The Author(s) 2024. Published by Oxford University Press on behalf of the Society for Neuro-Oncology.
Conflict of interest statement
A.L. is consultant and advisory board member for CCIE (not relevant to this study). A.A. is consultant and advisory board participant for Novartis (not relevant to this study). F.E. is advisory board participant for Servier and received honoraria from Dr. Sennewald Medizintechnik (not relevant to this study). S.M.P is consultant for Epignostix GbmH and BioSkryb (not relevant to this study). W.B. received honoraria from BMS, Novartis, and Roche (not relevant to this study). J.G. is consultant, advisory board participant and received honoraria for Novartis and Roche (not relevant to this study).
Figures





References
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
