

C-C Motif chemokine receptor-2 blockade ameliorates pulmonary hypertension in rats and synergizes with a pulmonary vasodilator
- PMID: 39556088
- PMCID: PMC12236072
- DOI: 10.1093/cvr/cvae244
C-C Motif chemokine receptor-2 blockade ameliorates pulmonary hypertension in rats and synergizes with a pulmonary vasodilator
Abstract
Aims: We investigated whether the disruption of C-C motif chemokine receptor (CCR) 2 may attenuate the development of pulmonary arterial hypertension (PAH) in any rat models with the reversal of the associated pro-inflammatory state and vascular dysfunction, and synergize with a conventional pulmonary vasodilator.
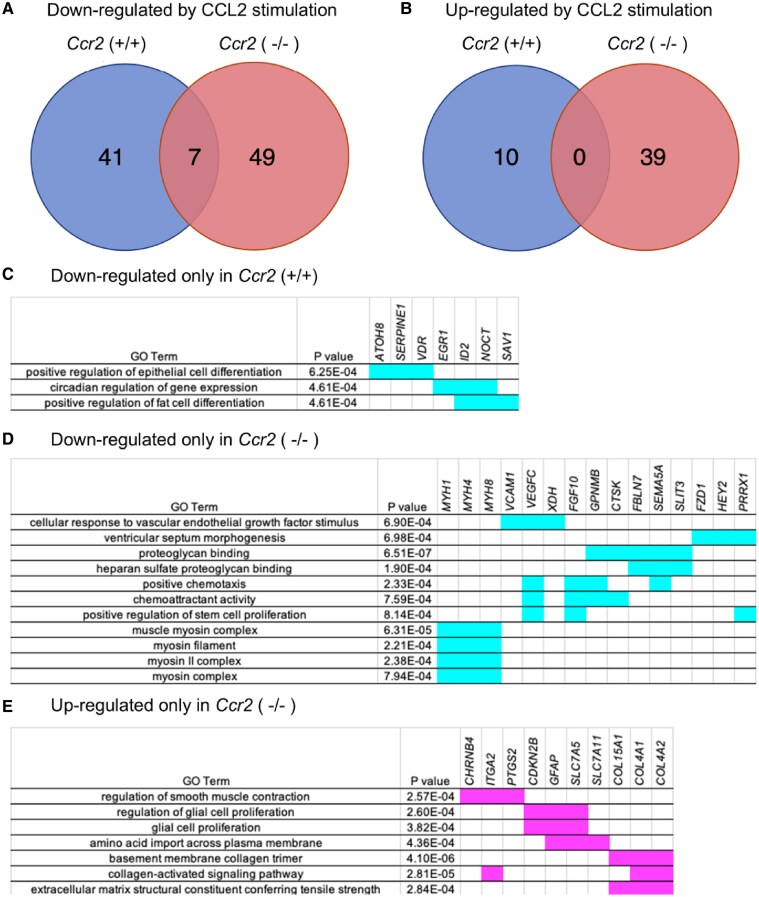
Methods and results: Using Ccr2(-/-) rats generated by CRISPR/Cas9, we investigated pulmonary hypertension (PH) in Ccr2(+/+) or Ccr2(-/-) rats treated with monocrotaline (MCT), SU5416/hypoxia (SuHx) and chronic hypoxia (CH). Ccr2(-/-) decreased the right ventricular systolic pressure, an index of right ventricular hypertrophy and mortality rate, and reversed increased expression of inflammatory cytokines/chemokines [interleukin-6, tumour necrosis factor-α, C-C motif chemokine receptor (CCL)-2, interleukin-1β, transforming growth factor-β] in rats 3weeks after MCT injection, but not in SuHx or CH models. Consistently, Ccr2(-/-) decreased indices of pulmonary vascular diseases (PVDs) and perivascular macrophage infiltration, as well as reversed impaired bone morphogenetic protein receptor type 2 signalling, increased endothelial apoptosis and impaired nitric oxide signalling and decreased phosphodiesterase-5 (PDE5) expression in lungs in MCT-treated rats. Gene expression of receptors for prostaglandin I2 and endothelin was not changed by Ccr2(-/-) in MCT-treated rats. In cultured pulmonary arterial smooth muscle cells (PASMCs), Ccr2(-/-) suppressed CCL2-induced hyperproliferation and dedifferentiation as well as reversed CCL2-induced decrease in PDE5 expression. The whole-genome RNA sequencing analysis identified differentially expressed genes in CCL2-stimulated Ccr2(-/-) PASMCs, which are related to the regulation of cellular differentiation and contraction. Based on studies in rats and cultured PASMCs, we investigated whether a PDE5 inhibitor, tadalafil, synergizes with Ccr2(-/-). Tadalafil administration ameliorated PH and PVDs in MCT-treated Ccr2(-/-) rats but not in Ccr2(+/+) rats. Tadalafil further improved survival in MCT-treated Ccr2(-/-) rats.
Conclusion: The present findings demonstrated that CCR2 disruption ameliorated PAH in MCT-treated rats, which was associated with the reversal of dysregulated inflammatory pathways and vascular dysfunction and synergized with tadalafil. These findings suggest that CCR2 may be a therapeutic target in intractable PAH patients with a certain CCR2-related inflammatory phenotype and refractory to conventional pulmonary vasodilators.
Keywords: Combination therapy; C–C Chemokine receptor type 2; Inflammation; Pulmonary hypertension.
© The Author(s) 2024. Published by Oxford University Press on behalf of the European Society of Cardiology.
Conflict of interest statement
Conflict of interest: none declared.
Figures







Comment in
-
C-C motif chemokine receptor 2 and phosphodiesterase type 5 inhibition in immune subphenotypes: a step toward personalized treatment for pulmonary arterial hypertension?Cardiovasc Res. 2025 Jul 8;121(7):980-982. doi: 10.1093/cvr/cvaf081. Cardiovasc Res. 2025. PMID: 40492521 No abstract available.
References
-
- Zelt JGE, Sugarman J, Weatherald J, Partridge ACR, Liang JC, Swiston J, Brunner N, Chandy G, Stewart DJ, Contreras-Dominguez V, Thakrar M, Helmersen D, Varughese R, Hirani N, Umar F, Dunne R, Doyle-Cox C, Foxall J, Mielniczuk L. Mortality trends in pulmonary arterial hypertension in Canada: a temporal analysis of survival per ESC/ERS guideline era. Eur Respir J 2021;59:2101552. - PMC - PubMed
MeSH terms
Substances
Grants and funding
- 22K07843/Ministry of Education, Culture, Sports, Science and Technology
- 18K07841/Ministry of Education, Culture, Sports, Science and Technology
- 20K08565/Ministry of Education, Culture, Sports, Science and Technology
- 18K08192/Ministry of Education, Culture, Sports, Science and Technology
- 17K11075/Ministry of Education, Culture, Sports, Science and Technology
LinkOut - more resources
Full Text Sources
Medical
