

Clinical Pharmacology of Cytokine Release Syndrome with T-Cell-Engaging Bispecific Antibodies: Current Insights and Drug Development Strategies
- PMID: 39556515
- PMCID: PMC11739781
- DOI: 10.1158/1078-0432.CCR-24-2247
Clinical Pharmacology of Cytokine Release Syndrome with T-Cell-Engaging Bispecific Antibodies: Current Insights and Drug Development Strategies
Abstract
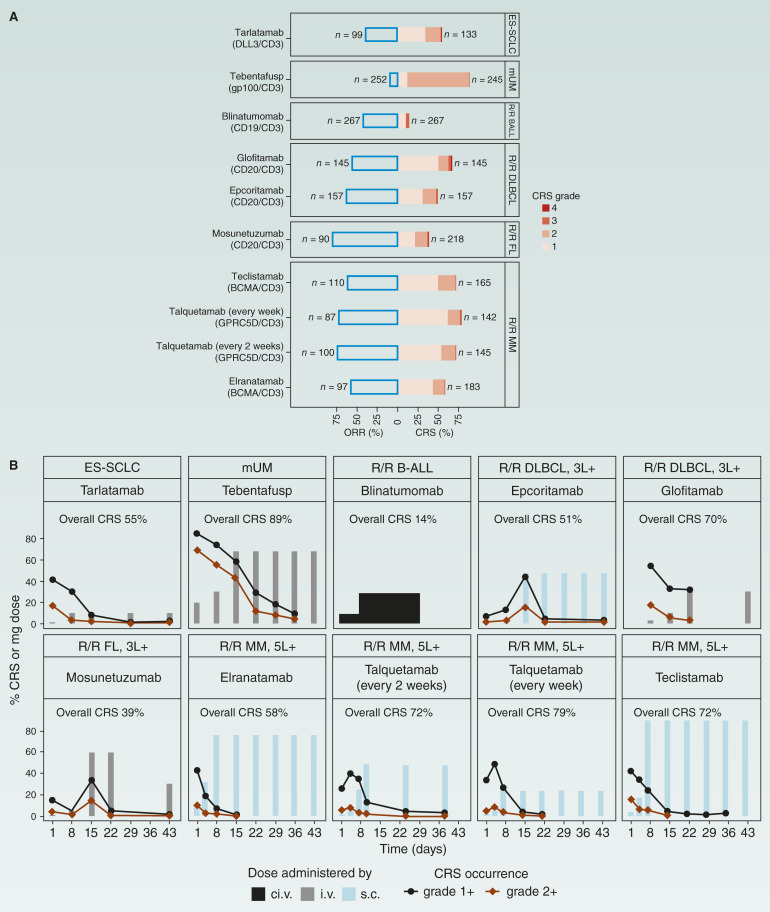
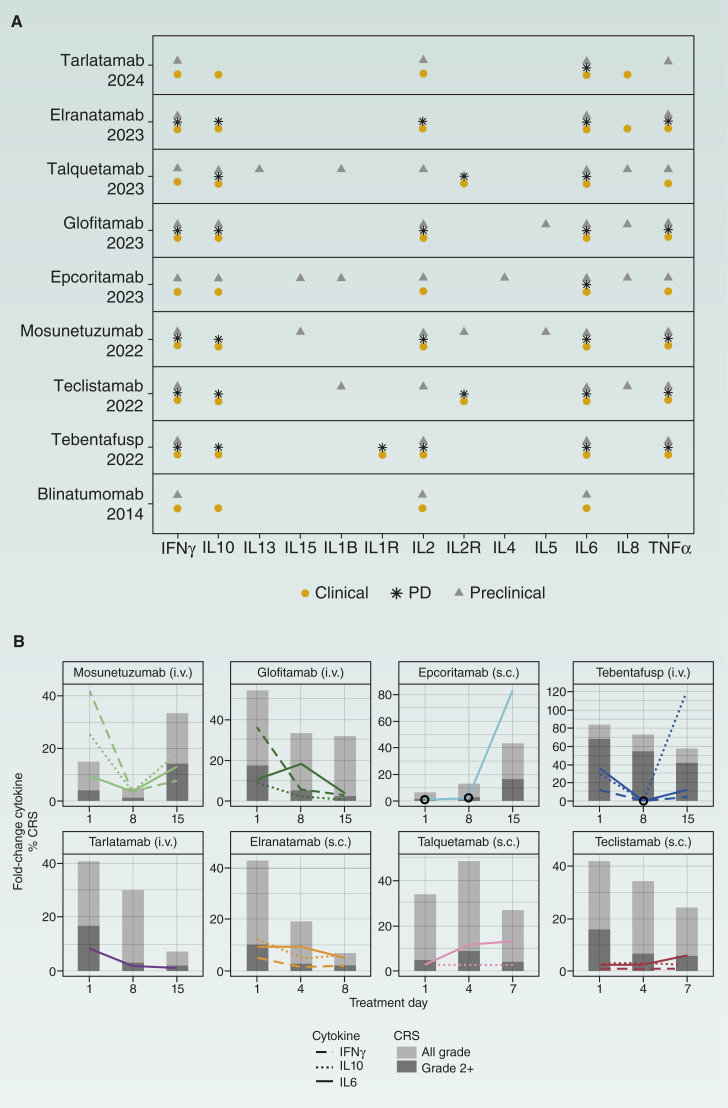
Cytokine release syndrome (CRS) is a common acute toxicity in T-cell therapies, including T-cell-engaging bispecific antibodies (T-BiSp). Effective CRS management and prevention are crucial in T-BiSp development. Required hospitalization for seven of the nine approved T-BiSp and the need for clinical intervention in severe cases highlight the importance of mitigation strategies to reduce health care burden and improve patient outcomes. In this review, we discuss the emerging evidence on CRS mitigation, management, and prediction. We cover different strategies for dose optimization, current and emerging (pre) treatment strategies, quantitative pharmacology tools used during drug development, and biomarkers and predictive factors. Insights are gleaned on step-up dosing and formulation effects on CRS and CRS relationships with cytokine dynamics and drug levels gathered through a review of T-BiSp licensing applications and emerging data from conferences and publications.
©2024 The Authors; Published by the American Association for Cancer Research.
Conflict of interest statement
K.K. Radtke reports employment with Genentech/Roche and ownership of Genentech/Roche shares. B.C. Bender reports current employment with Roche and ownership of Roche stock. Mosunetuzumab, a Roche molecule, is highlighted in the review. D.C. Turner reports other support from Roche/Genentech during the conduct of the study. S. Roy reports other support from Roche/Genentech outside the submitted work. A. Belousov reports personal fees from Hoffmann-La Roche Ltd. during the conduct of the study, as well as a patent for P36683-US-1 issued to Hoffmann-La Roche. C.-C. Li reports current employment with and stock ownership in Genentech/Roche. No disclosures were reported by the other author.
Figures
References
-
- Klein C, Brinkmann U, Reichert JM, Kontermann RE. The present and future of bispecific antibodies for cancer therapy. Nat Rev Drug Discov 2024;23:301–19. - PubMed
-
- Lee DW, Santomasso BD, Locke FL, Ghobadi A, Turtle CJ, Brudno JN, et al. . ASTCT consensus grading for cytokine release syndrome and neurologic toxicity associated with immune effector cells. Biol Blood Marrow Transplant 2019;25:625–38. - PubMed
-
- Hansen AR, Cook N, Amir E, Siu LL, Abdul Razak AR. Determinants of the recommended phase 2 dose of molecular targeted agents. Cancer 2017;123:1409–15. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
