

Preoperative goal directed therapy in geriatric hip fracture patients - a retrospective quality improvement study
- PMID: 39558199
- PMCID: PMC11571971
- DOI: 10.1186/s12877-024-05554-5
Preoperative goal directed therapy in geriatric hip fracture patients - a retrospective quality improvement study
Abstract
Background: Hip fractures in older adults are common and carry a high risk of morbidity and mortality. Preoperative dehydration, a key risk factor for adverse outcomes, is often underdiagnosed at admission. It is important to identify high risk patients and optimize modifiable risk factors to improve the postoperative outcome. The p-POSSUM Score is a useful predictor of postoperative mortality risk. Implementing a defined fluid resuscitation protocol early in high-risk groups has proven effective in reducing both postoperative morbidity and mortality.
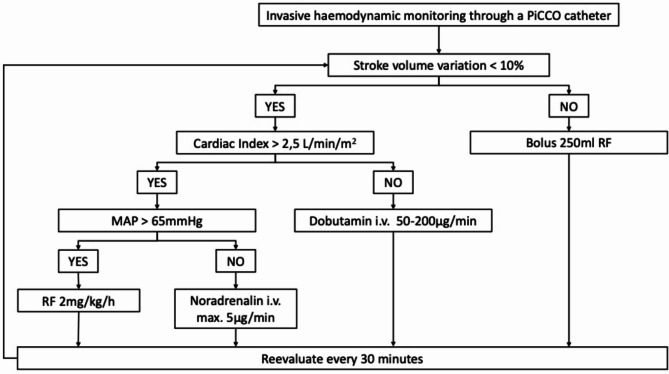
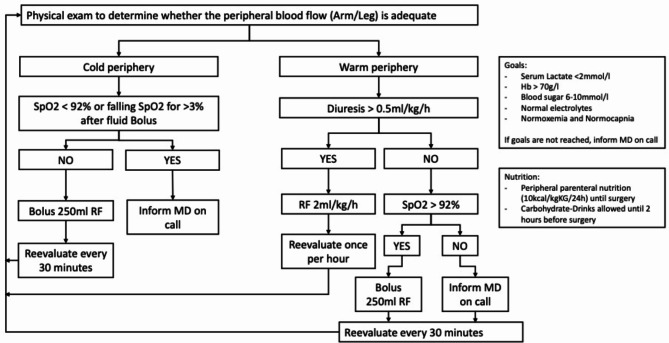
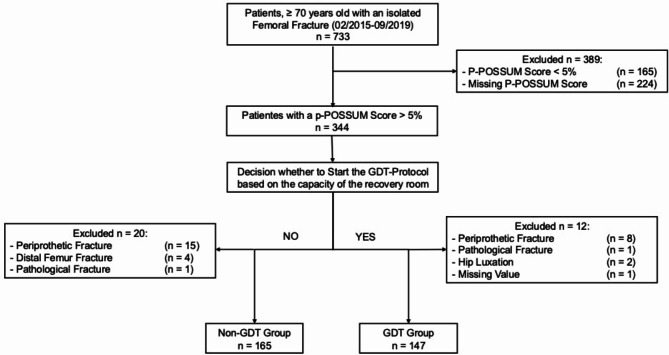
Materials and methods: We conducted a single-center, retrospective quality improvement study at a Level 1 trauma center in Switzerland, focusing on geriatric patients over 70 with a p-POSSUM Score > 5% and a proximal femur fracture, undergoing surgery between February 2015 and September 2019. We hypothesized that our institutional goal-directed fluid resuscitation protocol (GDT) would result in lower 30- and 90-day mortality rates and fewer complications for these high-risk patients. Outcome changes over time were analyzed annually.
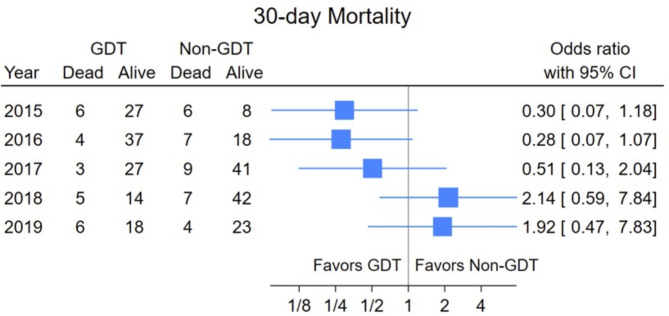
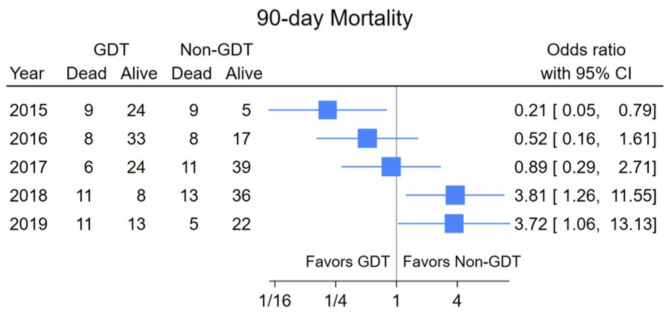
Results: 312 patients were included in our study. 147 followed our institutional GDT protocol, while 165 patients received standard care and were used as a control group. Initially, the odds ratio (OR) for 30-days mortality favored the GDT group; 2015 0.30 (CI: 0.07-1.18), 2016 0.28 (CI: 0.07-1.07), 2017 0.51 (CI: 0.13-2.04). This shifted toward the Non-GDT group in the year 2018 with a OR of 2.14 (CI: 0.59-7.84) and 2019 with 1.92 (CI 0.47-7.83). The pattern for 90-day mortality results was similar and slightly more pronounced. The estimates for the odds ratios remained consistent even after adjustment for the p-POSSUM score. The relative frequencies of complications showed no remarkable differences between the groups (GDT vs. Non-GDT).
Conclusion: In our study, the treatment according to our GDT protocol was associated with survival advantage in the first three years. However, this trend reversed in 2018, with Non-GDT patients faring better. Although our retrospective study does not provide enough evidence of causality between the protocol and the mortality rates, it revealed that continuous critical evaluation of internal processes is essential in healthcare for quality management. This allows timely identification and adaptation of processes to issues, especially after initially positive results.
Keywords: Geriatric trauma patients; Goal-directed therapy; Hip fracture; Quality improvement.
© 2024. The Author(s).
Conflict of interest statement
Figures
References
-
- Coburn M, Knobe ARM, Stevanovic A, Stoppe C, Rossaint R. Anesthesiological management of elderly trauma patients. Anaesthesist. 2016;65(2):98–106. - PubMed
-
- Bundesamt für Statistik S. D.u.M., Alterung der Bevölkerung. 2022.
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
