

Correlation between benign prostatic hyperplasia and comorbidities: a systematic analysis integrating global burden of disease and mendelian randomization study
- PMID: 39558312
- PMCID: PMC11575001
- DOI: 10.1186/s12967-024-05604-x
Correlation between benign prostatic hyperplasia and comorbidities: a systematic analysis integrating global burden of disease and mendelian randomization study
Abstract
Background: Benign prostatic hyperplasia (BPH) is a common chronic condition in elderly men. Observational studies have identified several comorbidities associated with BPH. However, these studies are limited by various confounding factors and do not clearly explain the association between BPH and its comorbidities. We investigated the association between BPH and comorbidities using the Global Burden of Disease (GBD) database combined with Mendelian randomization (MR) methods.
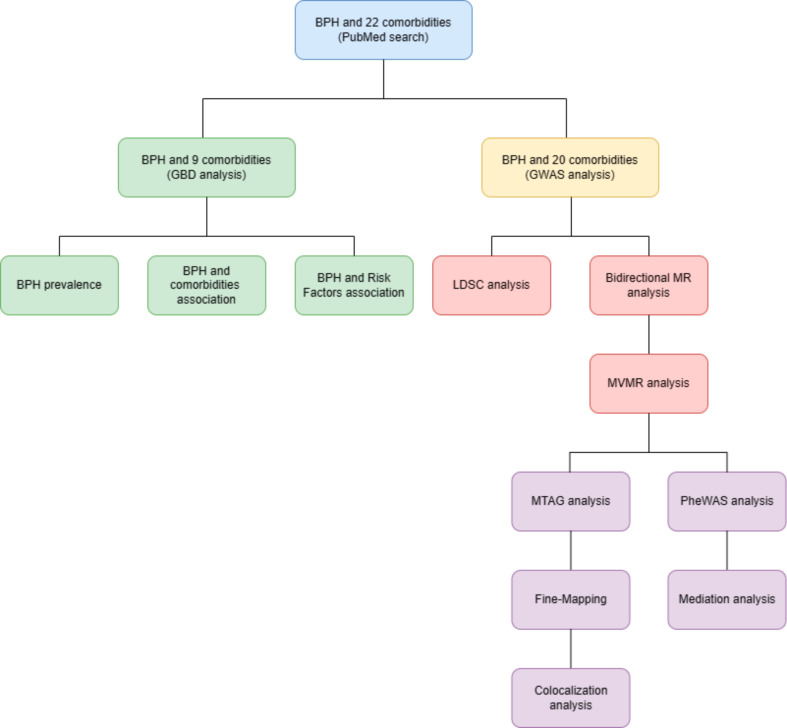
Methods: Through an extensive PubMed search, we identified 22 diseases associated with BPH and selected 9 significant comorbidities from the GBD database for a detailed correlation analysis. We also considered socio-economic and environmental influences on BPH. Utilizing the GWAS database, we gathered data on BPH and 20 comorbidities, employing the Linkage Disequilibrium Score Regression (LDSC) method to unearth genetic connections. Causality was determined through both univariable and multivariable bidirectional MR analyses, supplemented by Steiger directionality tests to confirm causation. The study's integrity was fortified by employing various MR models and conducting rigorous sensitivity analyses. The synthesis of GBD data with LDSC and MR findings offered a nuanced understanding of the BPH-comorbidity nexus. Additionally, we explored the genetic basis and the role of mediating factors between BPH and comorbidities through phenome-wide association studies (PheWAS), colocalization analysis, and mediation MR.
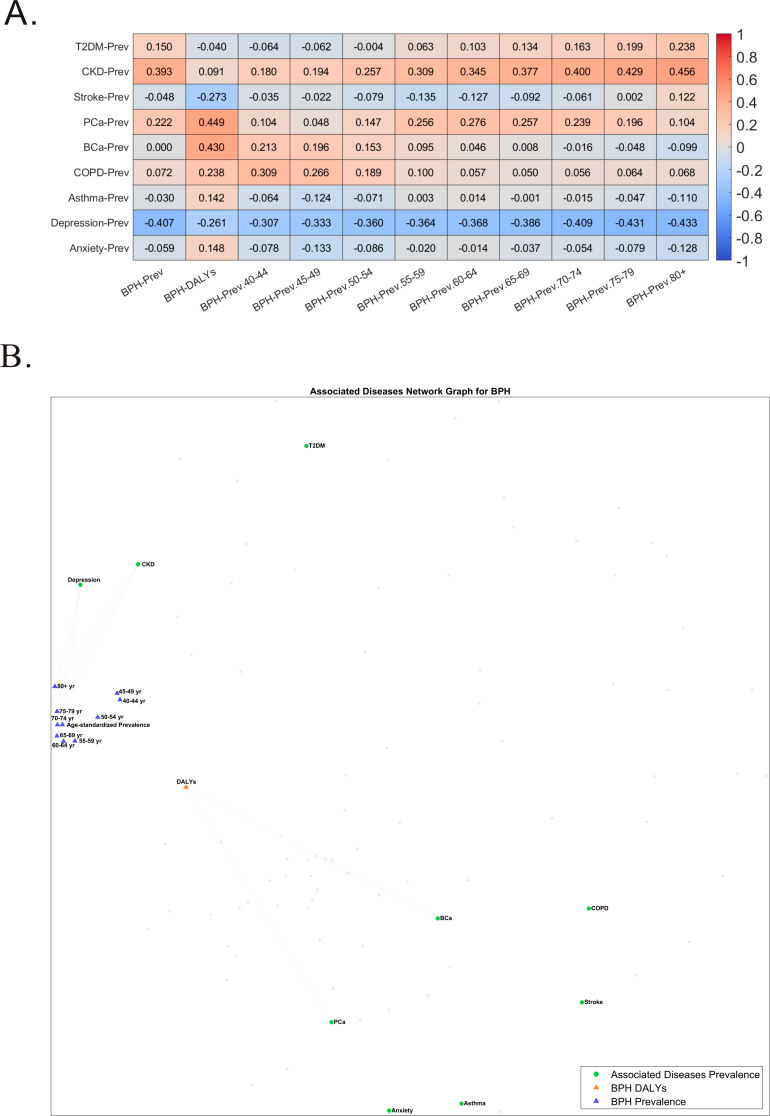
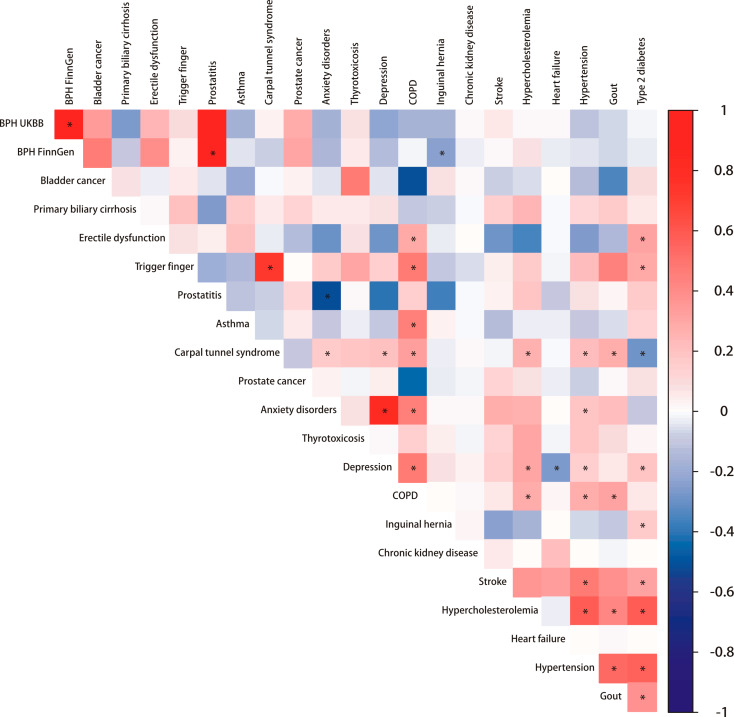
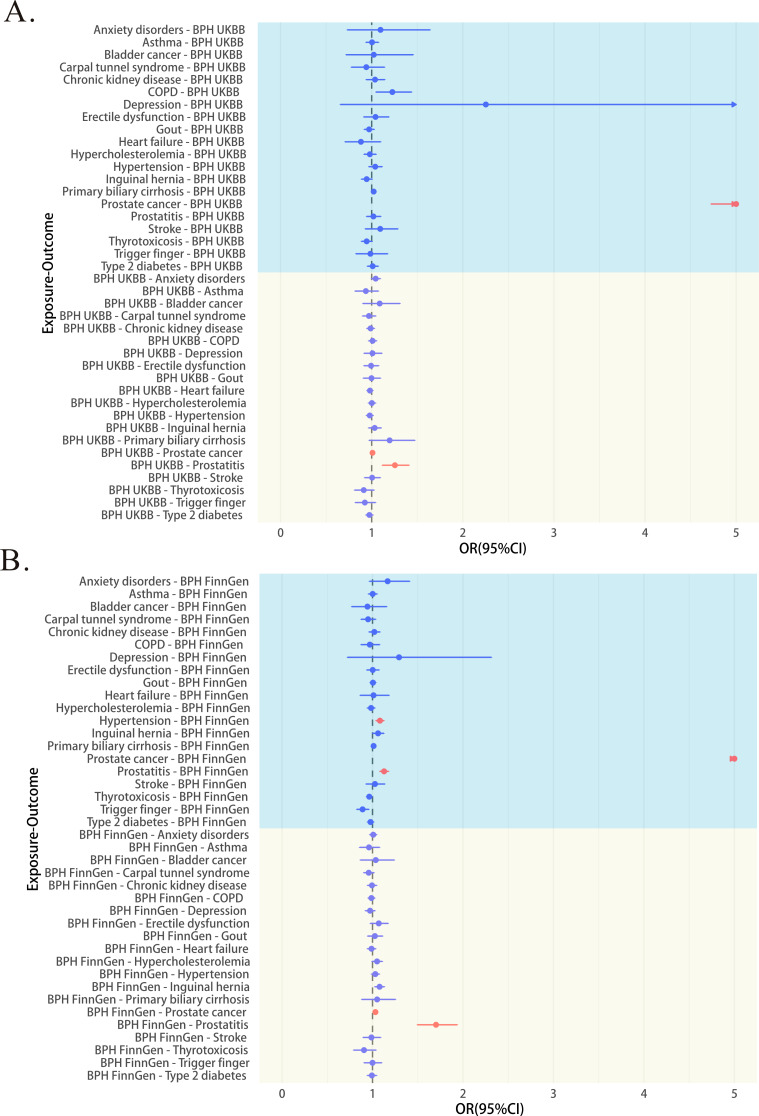
Results: Correlation analysis of GBD data found associations of prostate cancer, chronic kidney disease and depression with BPH. LDSC results indicated that prostatitis and bladder cancer are related to BPH. Two associations were replicated in bidirectional univariable MR, linking BPH with a higher risk of prostatitis and prostate cancer. conducted sensitivity analyses to confirm the robustness of the results and all Steiger directionality tests were correct. Multiple multivariable MR models validated these results. PheWAS analysis showed that outliers in MR do not significantly impact MR results. Through colocalization analysis, three shared loci between BPH and both prostatitis and prostate cancer were identified. Mediation analysis found that, after adjusting for BPH, fruit consumption was associated with a lower risk of prostatitis, and morning person and chronotype were associated with a lower risk of prostate cancer.
Conclusions: This study uncovered associations between BPH and various comorbidities, emphasizing the causal relationships between BPH, prostatitis, and prostate cancer. Our research provides a new perspective in understanding the comorbid associations of BPH.
Keywords: Benign prostatic hyperplasia; Causality; Comorbidities; Global burden of disease; Mendelian randomization analysis.
© 2024. The Author(s).
Conflict of interest statement
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
