

Nuclear medicine imaging in non-seminomatous germ cell tumors: lessons learned from the past failures
- PMID: 39558421
- PMCID: PMC11571929
- DOI: 10.1186/s40644-024-00794-5
Nuclear medicine imaging in non-seminomatous germ cell tumors: lessons learned from the past failures
Abstract
There is an unmet need for a more accurate molecular imaging radiotracer in the field of non-seminomatous germ cell tumors (NSGCT). The clinical problem is that no single imaging modality is able to differentiate teratoma from necrotic tissue in NSGCTs, which the nuclear medicine techniques are no exception. The exponential growth in the list of potentially promising radiotracers may hold promise in the future for imaging of NSGCTs. Here, we have reviewed the past efforts and potential future advances in this field.
Keywords: Imaging; Non-seminomatous germ cell tumor; Radiotracer; Retroperitoneal residual mass; Teratoma.
© 2024. The Author(s).
Conflict of interest statement
Figures



References
-
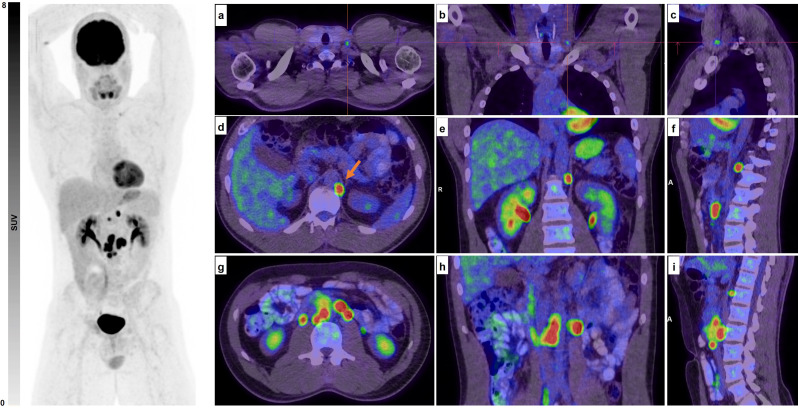
- Kaplan İ, Can C, Güzel Y, Alabalik U, Kömek H. 68 GA-FAPI-04 PET/CT Versus 18 F-FDG PET/CT in imaging of malignant mixed germ cell testicular tumor. Clin Nucl Med. 2023;48(4):e195–7. - PubMed
-
- Siegel RL, Miller KD, Wagle NS, Jemal A. Cancer statistics, 2023. CA Cancer J Clin. 2023;73(1):17–48. - PubMed
-
- Nallu A, Mannuel HD, Hussain A. Testicular germ cell tumors: biology and clinical update. Curr Opin Oncol. 2013;25(3):266–72. - PubMed
-
- Daneshmand S, Albers P, Fosså SD, Heidenreich A, Kollmannsberger C, Krege S, et al. Contemporary management of postchemotherapy testis cancer. Eur Urol. 2012;62(5):867–76. - PubMed
-
- Nauman M, Leslie SW. Nonseminomatous Testicular Tumors. StatPearls. Treasure Island (FL): StatPearls Publishing Copyright © 2024. StatPearls Publishing LLC.; 2024. - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
