

Clinical Characteristics of Steatotic Liver Disease Categories in a Large Cohort of Japanese Health Checkup Participants
- PMID: 39559296
- PMCID: PMC11570837
- DOI: 10.1016/j.gastha.2024.08.006
Clinical Characteristics of Steatotic Liver Disease Categories in a Large Cohort of Japanese Health Checkup Participants
Abstract
Background and aims: The clinical characteristics and risk factors involved in the development of liver fibrosis in the subtypes of steatotic liver disease (SLD) remain unknown. We examined the clinical characteristics of SLD subtypes using a large Japanese cohort.
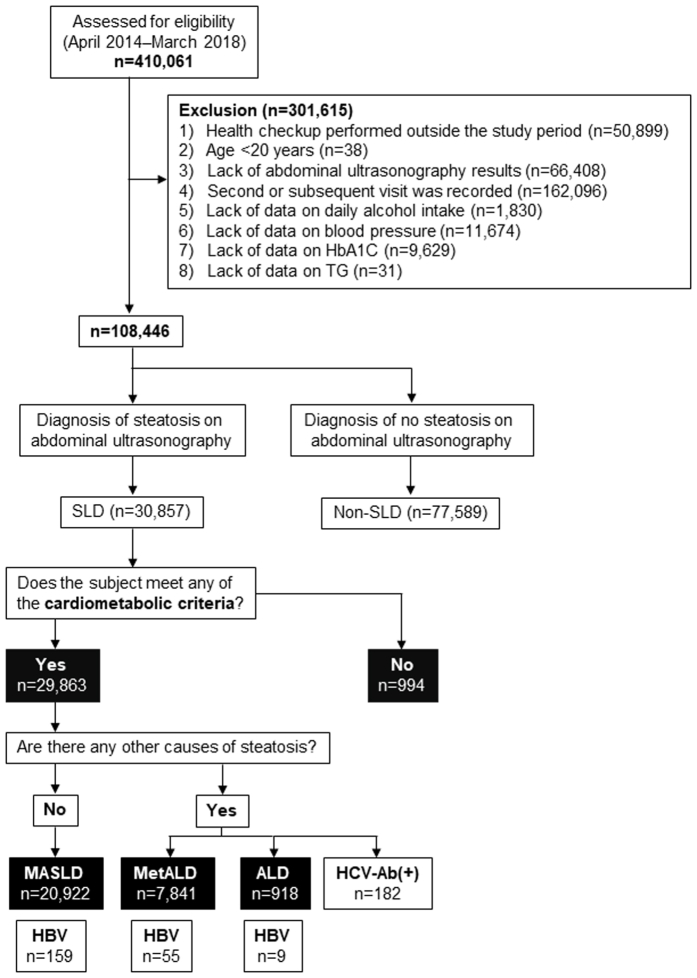
Methods: We performed a cross-sectional analysis (total n = 108,446). In this cohort, SLD was diagnosed by ultrasonography. Individuals with none of the cardiometabolic risk factors were excluded.
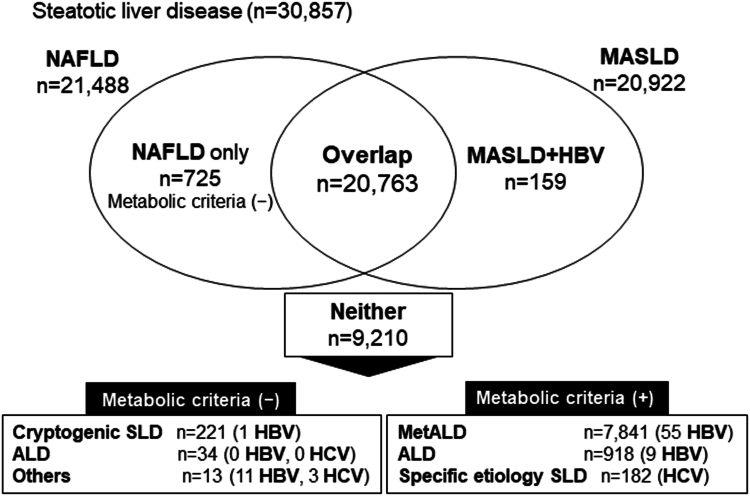
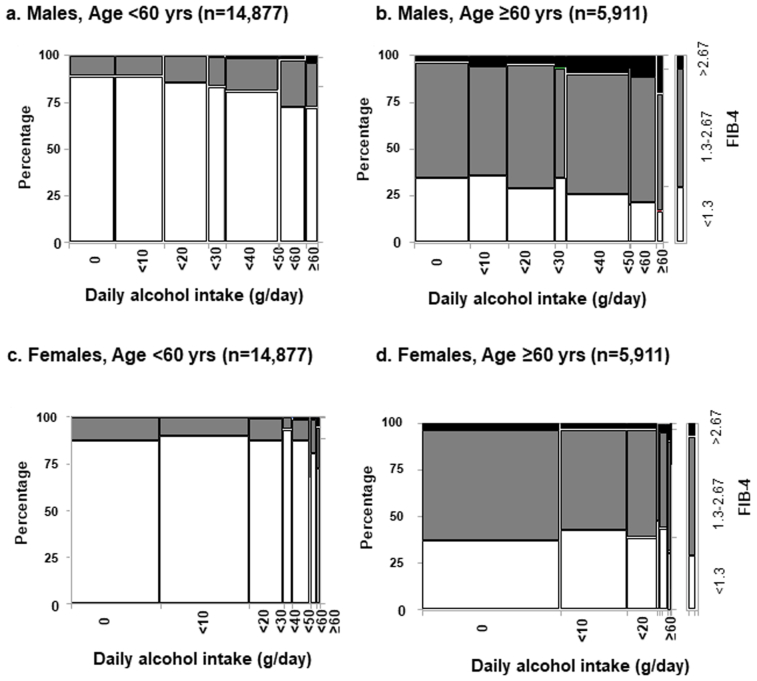
Results: According to their nonalcoholic fatty liver disease (NAFLD) and metabolic dysfunction-associated steatotic liver disease (MASLD) status based on the database, participants with cardiometabolic criteria were allocated to the MASLD, MASLD with increased alcohol intake (MetALD), and alcohol-associated liver disease (ALD) with metabolic dysfunction groups. Of 30,857 subjects with SLD, 21,488 (69.6%) had NAFLD, and 20,922 (67.8%) had MASLD. There were few differences in the clinical characteristics between NAFLD and MASLD. After adjustment for clinical variables, we found that male patients with MetALD [odds ratio (OR) 2.26; 95% confidence interval (CI) 1.87-2.84] and ALD with metabolic dysfunction (OR 3.92; 95% CI 2.85-5.39) had a significantly higher risk for advanced liver fibrosis (diagnosed by Fibrosis-4 (FIB-4) index >2.67) compared to those with MASLD. In female patients with ALD, metabolic dysfunction (OR 5.80; 95% CI 2.51-13.4) and systemic blood pressure of ≥130 mmHg were significant risk factors for high FIB-4 (males: OR 3.38, 95% CI 2.51-4.55; females: OR 4.34, 95% CI 2.66-7.07, P < .001).
Conclusion: Alcohol intake and systolic blood pressure are independent contributors to liver fibrosis progression assessed by FIB-4 in SLD.
Keywords: Alcohol Intake; FIB-4 Index; Metabolic Dysfunction; Steatotic Liver Disease; Systolic Blood Pressure.
© 2024 Published by Elsevier Inc. on behalf of the AGA Institute.
Figures
References
-
- Younossi Z.M., Wong G., Anstee Q.M., et al. The global burden of liver disease. Clin Gastroenterol Hepatol. 2023;21(8):1978–1991. - PubMed
-
- Song S.J., Che-To Lai J., Lai-Hung Wong G., et al. Can we use old NAFLD data under the new MASLD definition? J Hepatol. 2024;80(2):e54–e56. - PubMed
-
- Li M., Xie W. Are there all-cause mortality differences between metabolic dysfunction-associated steatotic liver disease subtypes? J Hepatol. 2024;80(2):e53–e54. - PubMed
-
- Von Elm E., Altman D.G., Egger M., et al. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. Int J Surg. 2014;12(12):1495–1499. - PubMed
LinkOut - more resources
Full Text Sources
