Adrenal Hemorrhage as a Complication of Plug-assisted Retrograde Transvenous Obliteration of Gastrorenal Shunt Managed by Adrenal Artery Embolization: A Case Report
- PMID: 39559814
- PMCID: PMC11570214
- DOI: 10.22575/interventionalradiology.2023-0032
Adrenal Hemorrhage as a Complication of Plug-assisted Retrograde Transvenous Obliteration of Gastrorenal Shunt Managed by Adrenal Artery Embolization: A Case Report
Abstract
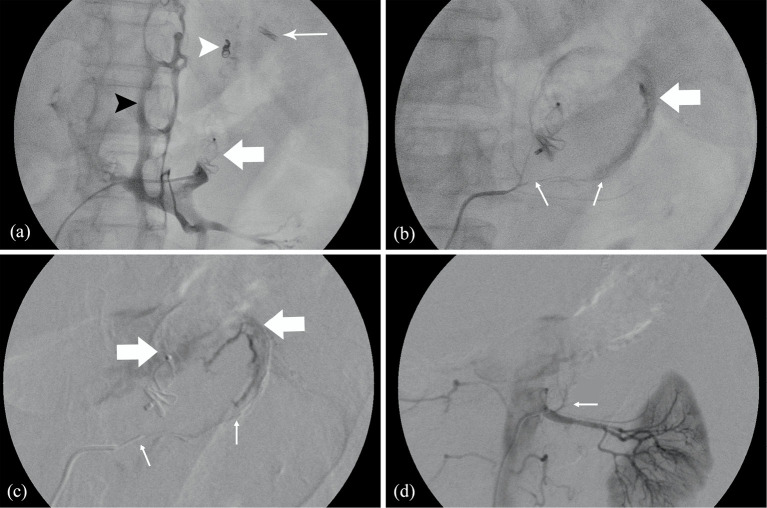
We describe a patient who underwent plug-assisted retrograde transvenous obliteration for gastric varices. After the procedure, the patient developed hypotension and tachycardia. Contrast-enhanced computed tomography showed a left adrenal hematoma. The patient was managed with left inferior adrenal artery embolization. We herein describe an unexpected complication during plug-assisted retrograde transvenous obliteration and the endovascular management by adrenal artery embolization. We speculate that inadvertent cannulation of an adrenal vein tributary and iatrogenic trauma thereafter caused by sheath advancement was a probable cause for this complication. Further increase in intra-adrenal pressure due to blockage of the adrenal vein outflow postplug deployment possibly led to the rupture of adrenal vein tributary and adrenal gland hematoma in our case.
Keywords: adrenal artery embolization; adrenal hemorrhage; chronic liver disease (CLD); plug-assisted retrograde transvenous obliteration (PARTO); portal hypertension.
© 2024 Japanese Society of Interventional Radiology.
Conflict of interest statement
None
Figures