

Evaluation of waning of IgG antibody responses after rVSVΔG-ZEBOV-GP and Ad26.ZEBOV, MVA-BN-Filo Ebola virus disease vaccines: a modelling study from the PREVAC randomized trial
- PMID: 39559990
- PMCID: PMC11632942
- DOI: 10.1080/22221751.2024.2432353
Evaluation of waning of IgG antibody responses after rVSVΔG-ZEBOV-GP and Ad26.ZEBOV, MVA-BN-Filo Ebola virus disease vaccines: a modelling study from the PREVAC randomized trial
Abstract
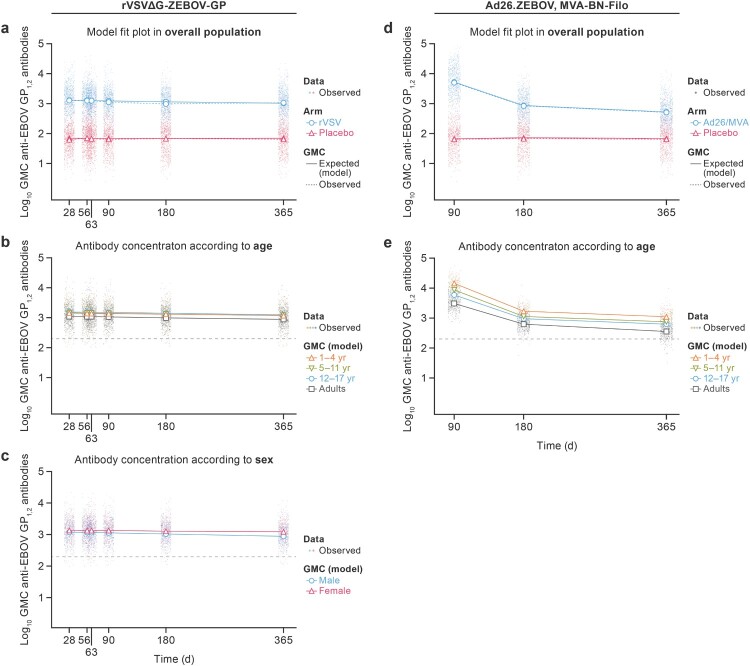
rVSVΔG-ZEBOV-GP and Ad26.ZEBOV, MVA-BN-Filo are WHO-prequalified vaccination regimens against Ebola virus disease (EVD). Challenges associated with measuring long-term clinical protection warrant the evaluation of immune response kinetics after vaccination. Data from a large phase 2 randomized double-blind clinical trial (PREVAC) were used to evaluate waning of anti-Ebola virus (EBOV) glycoprotein (GP1,2) antibody concentrations after rVSVΔG-ZEBOV-GP or Ad26.ZEBOV, MVA-BN-Filo vaccination with linear mixed-effect regression models. After a post-vaccination peak, each vaccination strategy was associated with a decrease of anti-EBOV GP1,2 antibody concentrations with distinct kinetics, highlighting a less-rapid decline in antibody levels after vaccination by rVSVΔG-ZEBOV-GP. One year after administration of the vaccine, antibody concentrations were higher in children compared to adults for both vaccines, although with different effect sizes: 1.74-fold higher concentrations (95% confidence interval [CI] [1.48; 2.02]) for children 12-17 years old to 3.10-fold higher concentrations (95% CI [2.58; 3.69]) for those 1-4 years old compared to adults for Ad26.ZEBOV, MVA-BN-Filo versus 1.36-fold (95% CI [1.12; 1.61]) to 1.41-fold (95% CI [1.21; 1.62]) higher than these values for adults, with relatively small changes from one age category of children to another, for rVSVΔG-ZEBOV-GP. Antibody concentrations also differed according to geographical location, pre-vaccination antibody concentration, and sex. In combination with knowledge on memory response, characterization of the major determinants of immune response durability of both vaccinations may guide future EVD control protocols.Trial registration: ClinicalTrials.gov identifier: NCT02876328.
Keywords: Ebola virus disease; Western Africa; antibody; immunogenicity; modelling; vaccine.
Conflict of interest statement
No potential conflict of interest was reported by the author(s).
Figures
References
-
- Kuhn JH, Amarasinghe GK, Perry DL.. Filoviridae. In: Howley PM, Knipe DM, Whelan SPJ, editors. Fields virology. Vol. 1, Emerging viruses. 7th ed. Philadelphia (PA: ): Wolters Kluwer/Lippincott Williams & Wilkins; 2020. p. 449–503.
-
- European Medicines Agency . Ebola; 2022. Available from: https://www.ema.europa.eu/en/human-regulatory/overview/public-health-thr...
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical