

Multimodal treatment of glioblastoma with multiple lesions - a multi-center retrospective analysis
- PMID: 39560695
- PMCID: PMC11614972
- DOI: 10.1007/s11060-024-04810-3
Multimodal treatment of glioblastoma with multiple lesions - a multi-center retrospective analysis
Abstract
Objective: The presence of multiple localizations (ML) in glioblastoma is rare and associated with perceived poor prognosis. The aim of this study is to evaluate the impact of a multimodal treatment on progression-free survival (PFS) and overall survival (OS) in ML glioblastoma.
Methods: Patients presenting with CNS WHO grade 4 glioblastoma with ML to 2 major German Departments of Neurosurgery between January 1st, 2008, to December 31st, 2020 were included in this study. Primary outcome parameters were extent of resection (EOR) using the 2021 RANO criteria, progression free- and overall survival.
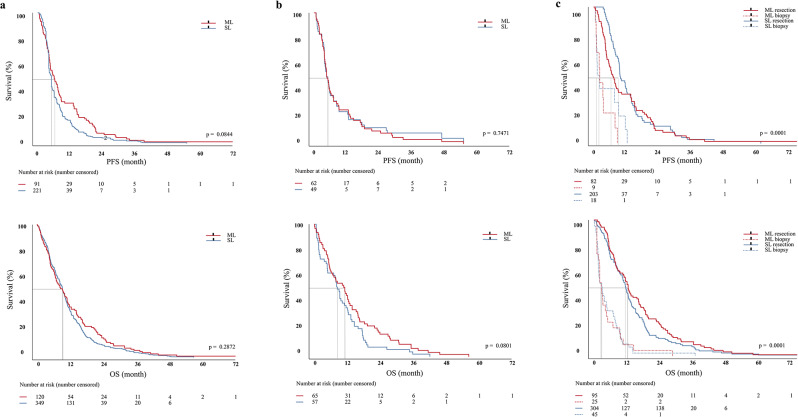
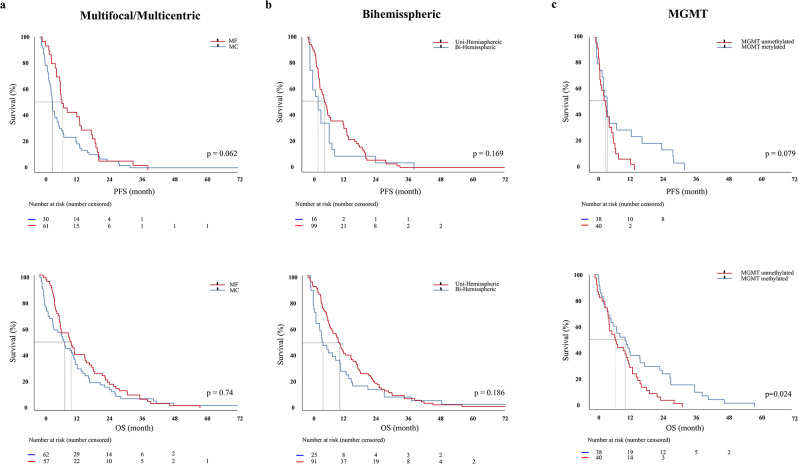
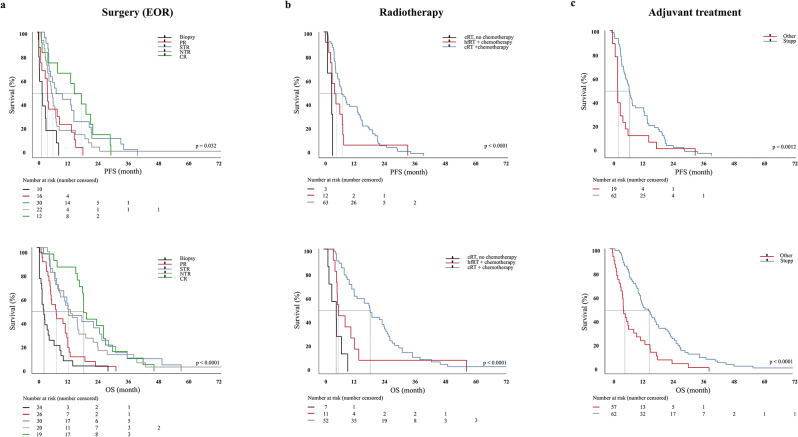
Results: A total of 483 patients with newly diagnosed glioblastoma (CNS WHO grade 4) were assessed. 134 patients presented with ML (72 multifocal (MF), 62 multicentric (MC)). The median PFS and OS did not differ among MC and MF glioblastomas. The EOR was a significant predictor of PFS and OS in ML glioblastoma. complete-, near total-, and subtotal resection significantly prolonged PFS (p < 0.0001) and OS (p < 0.0001) compared to biopsy alone. Standard radiotherapy (p = 0.045) and hypofractionated (p < 0.0001) radiotherapy and adjuvant treatment (Stupp protocol) prolonged PFS (p = 0.0012) and OS (p < 0.0001). In multivariate analysis Karnfosky performance score, EOR, and concomitant adjuvant treatment remained significant factors influencing OS. Propensity score matching of patients with ML and solitary lesion tumors showed similar PFS and OS (p = 0.08).
Conclusion: The presented data suggests that glioblastomas with multiple lesions treated with multimodal therapy equal survival rates compared to patients with solitary lesion tumors can be achieved. The results reflect the importance of an equally aggressive maximal treatment effort in this particular and often marginalized group of patients.
• Multifocal and multicentric glioblastoma are the same entity according to their clinical course. • EOR and adjuvant treatment are the most important predictors of PFS and OS in multiple lesion glioblastoma. • Multiplelesion- and solitary lesion glioblastoma have similar survival rates if treated equally.
Keywords: Extent of resection; Glioblastoma; Multicentric; Multifocal; Multimodal therapy.
© 2024. The Author(s).
Conflict of interest statement
Declarations. Ethical approval: The ethics committee of Rhineland-Palatinate, Germany, reviewed and approved this study (No: 2020-15140-retrospektiv). Competing interests: The authors declare no competing interests.
Figures
References
-
- Alexander BM, Cloughesy TF (2017) Adult glioblastoma. J Clin Oncol 35(21):2402–2409 - PubMed
-
- Stupp R, Mason WP, Van Den Bent MJ et al (2005) Radiotherapy plus Concomitant and Adjuvant Temozolomide for Glioblastoma. N Engl J Med 352(10):987–996 - PubMed
-
- Dono A, Wang E, Lopez-Rivera V et al (2020) Molecular characteristics and clinical features of multifocal glioblastoma. J Neurooncol 148(2):389–397 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
