

ER + HER2- early-stage breast cancer: association of HER2 expression, tumor characteristics, and outcomes
- PMID: 39560822
- PMCID: PMC12353014
- DOI: 10.1007/s10549-024-07549-7
ER + HER2- early-stage breast cancer: association of HER2 expression, tumor characteristics, and outcomes
Abstract
Purpose: To evaluate the association between the HER2 score as provided by the Oncotype DX Recurrence Score (RS) assay, tumor characteristics, and outcomes in early-stage, ER + HER2-negative breast cancer (BC).
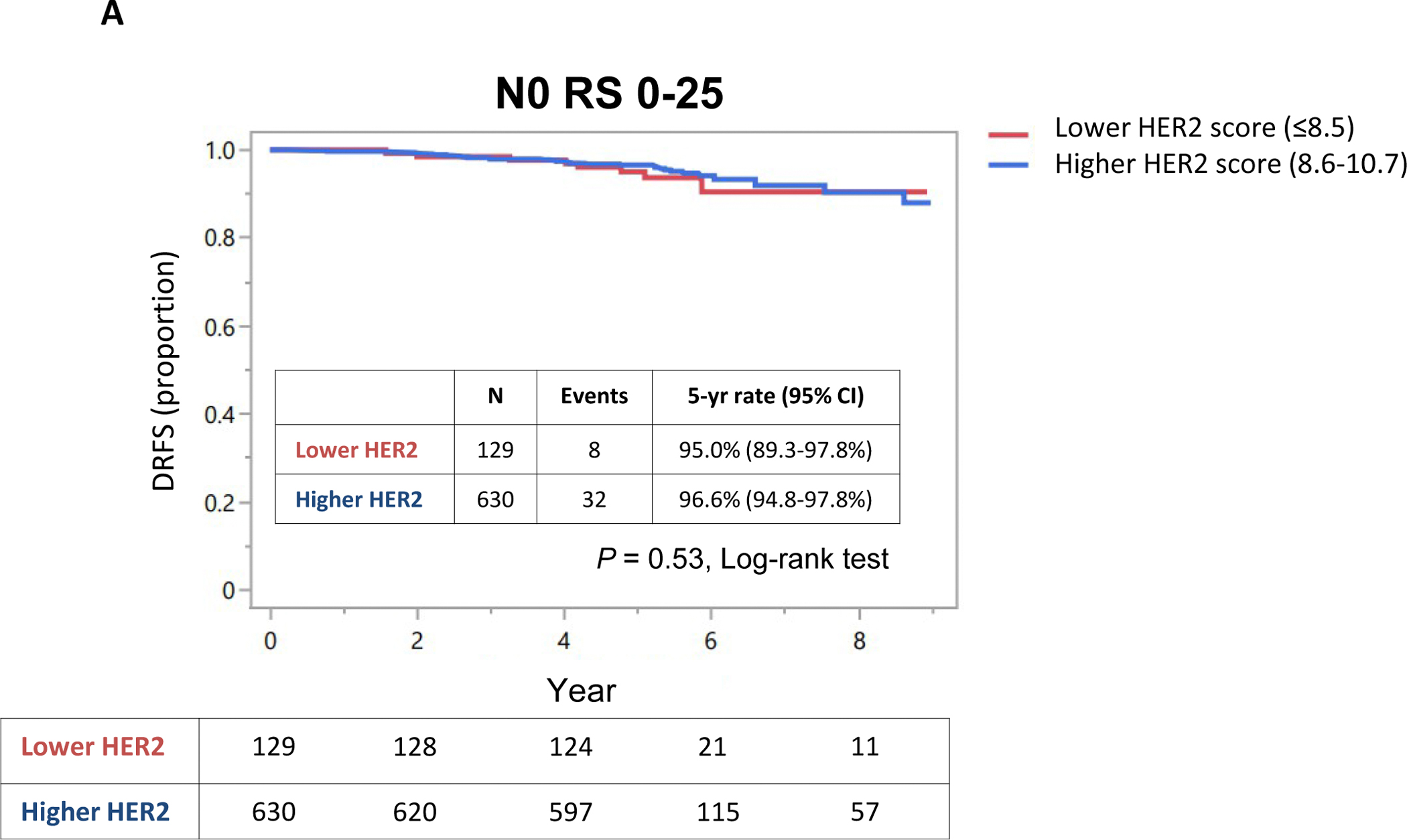
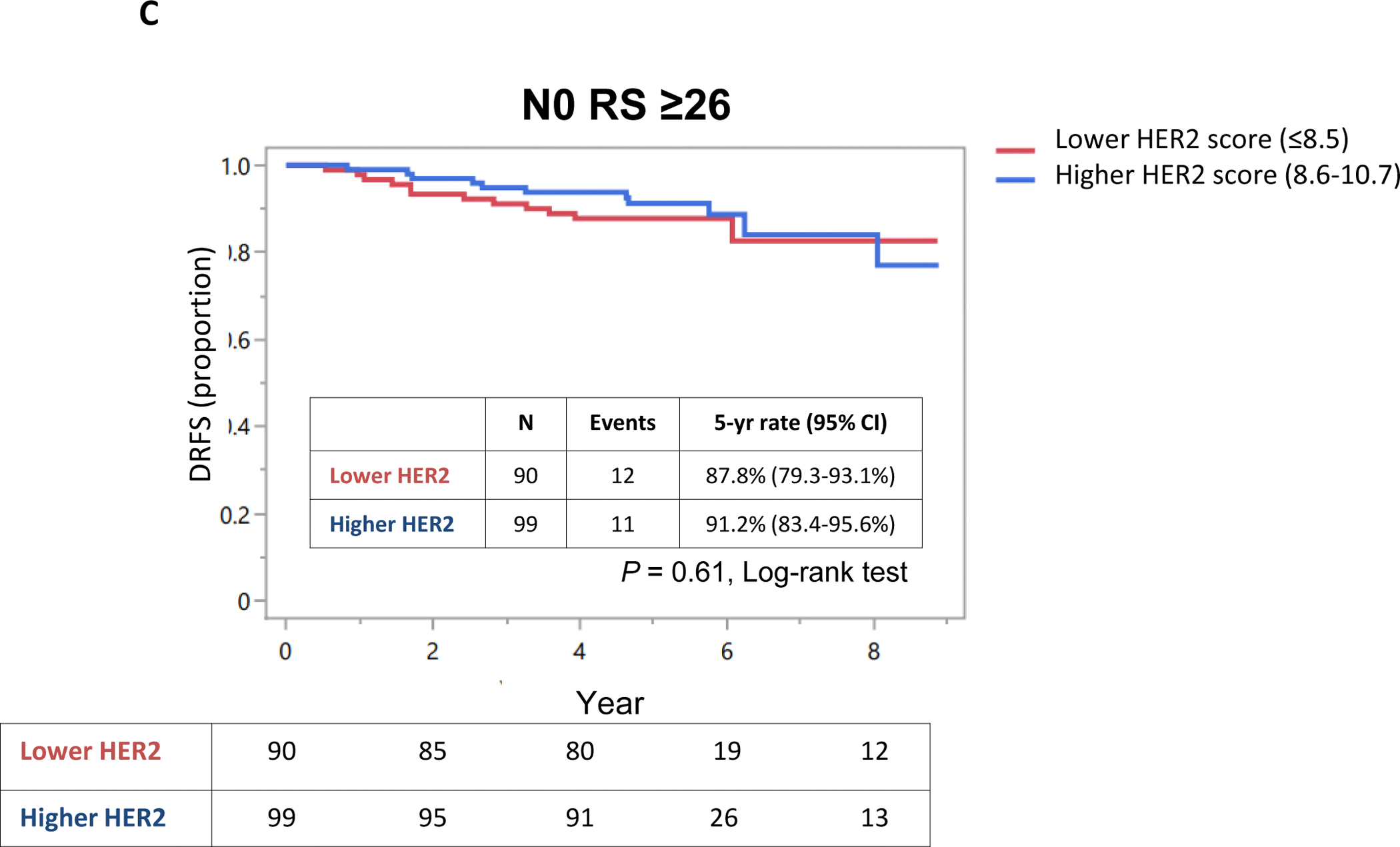
Methods: All women insured by the Clalit Health Services, with early-stage, ER + HER2-negative BC who underwent RS testing between 2008 and 2011 were included. Patient/tumor characteristics and Kaplan-Meier estimates for distant recurrence-free survival (DRFS) and overall survival (OS) were compared by HER2 category, based on the HER2 score provided by the RS assay: lower HER2 score group representing the lower third of the HER2 score range (≤ 8.5); higher HER2 score group representing the upper 2 thirds of the HER2 score range (8.6-10.7).
Results: 1535 patients were included (948 node negative, 587 node positive); 330 (21.5%) were categorized as lower HER2 score and 1205 (78.5%) as higher HER2 score. Compared to the higher HER2 score group, the lower score group included a significantly higher proportion of patients with RS ≥ 26 in both node-negative (41% vs. 13.6%, P < .001) and node-positive diseases (36% vs. 19.4%, P < .001). Compared to the higher HER2 score group, the lower score group had significantly lower Oncotype ER and PR scores and lower proportion of lobular disease. Age and tumor size were comparable between the HER2 score groups. Within each RS category, DRFS and OS were not associated with the HER2 score.
Conclusion: Lower HER2 score was associated with higher RS results. Further study is desired to elucidate the role and significance of HER2 expression in early-stage, ER + HER2-negative.
Keywords: HER2 mRNA; HER2-low; Oncotype; Recurrence score.
© 2024. The Author(s), under exclusive licence to Springer Science+Business Media, LLC, part of Springer Nature.
Conflict of interest statement
Declarations. Competing interests: Author HG reports personal fee from: AstraZeneca (Honorarium), Gilead (Honorarium and consulting), Eli-Lilly (Honorarium and consulting), MSD (Honorarium and consulting), Novartis (Honorarium and consulting), Pfizer (Honorarium and consulting), Roche (Honorarium), Rhenium Oncotest (Honorarium and consulting), all not related to the submitted manuscript. Author RY reports personal fees from: Roche (consulting, invited speaker, Research grant), Pfizer (consulting), Novartis (consulting, invited speaker), Rhenium (consulting), Medison (invited speaker), MSD (consulting, invited speaker), Astra-Zeneca (consulting, invited speaker), Eli Lilly (consulting, invited speaker), Gilead (consulting), Stemline (invited speaker, consulting) all not related to submitted manuscript. Author SPS reports: Roche (consultancy, advisory board, speaker's bureau, travel grant), Novartis (consultancy, advisory board, speaker's bureau), Pfizer (consultancy, advisory board, speaker's bureau, travel grant, Institutional independent research grant), Astra-Zeneca (consultancy, advisory board, speaker's bureau), Gilead (consultancy, advisory board, speaker's bureau, travel grant), Eli Lily (consultancy, advisory board, speaker's bureau), MSD (consultancy, advisory board, speaker's bureau), Stemline (consultancy), all via institutional fees and not related to the submitted manuscript. Author AS reports: Roche(consultancy, advisory board, speaker's bureau, travel grant), Novartis (consultancy, advisory board, speaker's bureau), Pfizer (consultancy, advisory board, speaker's bureau, travel grant, institutional independent research grant), Astra-Zeneca (consultancy, advisory board, speaker's bureau), Gilead (consultancy, advisory board, speaker's bureau, travel grant), Lily (consultancy, advisory board, speaker's bureau), MSD (consultancy, advisory board, speaker's bureau), Stemline (consultancy), all via institutional fees and not related to the submitted manuscript. Author AS reports: Eli Lilly (consulting, advisory board, speakers bureau), Pfizer (consulting, advisory board, speakers bureau), Roche (consulting, advisory board, speakers bureau, research grant), Novartis (consulting, advisory board, speakers bureau, research grant), Gilead (consulting, advisory board), MSD (consulting, advisory board, speakers bureau, travel grant), Astra-Zenca (consulting, advisory board), Progenetics (consulting, advisory board), Rhenium (consulting, advisory board), Neopharm (travel grant), Celgene (travel grant), Medison (travel grant), all not related to the submitted work. Author ABS reports being a consultant for Oncotest Rhenium, and Exact Sciences, related to the submitted manuscript, and to Pfizer, Can-Fite, and MDI, not related to the submitted manuscript. Author SMS reports: research grant from Can-Fite, AstraZeneca, Bioline RX, BMS, Halozyme, Clovis Oncology, CTG Pharma, Exelexis, Geicam, Halozyme, Incyte, Lilly, Moderna, Teva pharmaceuticals, and Roche, and owning stocks and options in CTG Pharma, DocBoxMD, Tyrnovo, VYPE, Cytora, and CAN-FITE, all not related to the submitted manuscript. All other authors have no conflicts of interest. This study was funded by Oncotest-Rhenium. The funder played no role in the design and conduct of the analysis or its interpretation, and the decision to submit the manuscript for publication.
Figures










References
-
- NCCN Guidelines. https://www.nccn.org/professionals/physician_gls/pdf/breast.pdf, accessed March 2024.
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
