

Comparison of autologous matrix-induced chondrogenesis and mosaicplasty in the treatment of osteochondral defects of the talus
- PMID: 39560972
- PMCID: PMC11583942
- DOI: 10.5152/j.aott.2024.23001
Comparison of autologous matrix-induced chondrogenesis and mosaicplasty in the treatment of osteochondral defects of the talus
Abstract
Objective: This study aimed to compare the medium- to long-term results of mosaicplasty and autologous matrix-induced chondrogenesis (AMIC) in treating osteochondral defects of the talus (OCD).
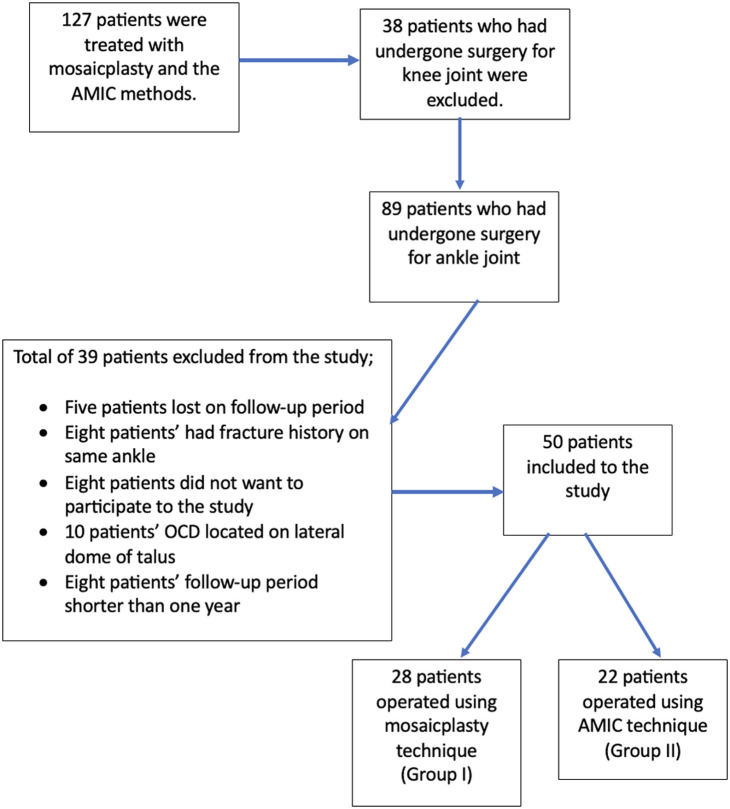
Methods: Fifty patients treated for talus OCD were evaluated between 2010 and 2020. Patients were divided into 2 groups: patients who underwent mosaicplasty (Group I) and those who underwent AMIC (Group II). The OCD was graded according to the Berndt-Hardy and Hepple classification systems. The size of the OCD area, the number of osteochondral plugs, and the size of the collagen matrix were determined from the surgical data. The effects of patients aged below and above 45, defect areas smaller or larger than 1.5 cm2 , and gender on functional outcomes were analyzed in both groups. Range of motion (ROM), The American Orthopaedic Foot & Ankle Society score (AOFAS), the Freiburg ankle Index score (FAI), the Tegner activity scale, and the visual analog scale (VAS) were used for the functional evaluations.
Results: Group I included 28 patients, and group II included 22 patients. The mean age was 41.6 years; the mean follow-up period was 69.9 months. In the final examination of the patients, both methods could provide significant improvement in all functional scores (P < .001). Although it was not statistically significant, group II had better functional values. The size of the defect area independently negatively affected the preoperative AOFAS (P=.001 and P=.011, respectively) and FAI (P=.001 and P=.008, respectively) scores. Besides that, age and gender did not affect the results (P > .05).
Conclusion: Both methods can provide successful results; however, the AMIC method can achieve better results than mosaicplasty in similarly sized defects without causing additional morbidity.
Keywords: Autologous; Chondrogenesis; Mosaicplasty; Osteochondral defects; Talus.
Conflict of interest statement
Figures




Similar articles
-
Reconstruction of osteochondral lesions of the talus with autologous spongiosa grafts and autologous matrix-induced chondrogenesis.Am J Sports Med. 2013 Mar;41(3):519-27. doi: 10.1177/0363546513476671. Epub 2013 Feb 7. Am J Sports Med. 2013. PMID: 23393079
-
Autologous Matrix-Induced Chondrogenesis for Osteochondral Lesions of the Talus: A Clinical and Radiological 2- to 8-Year Follow-up Study.Am J Sports Med. 2019 Jun;47(7):1679-1686. doi: 10.1177/0363546519841574. Epub 2019 May 14. Am J Sports Med. 2019. PMID: 31084491
-
Arthroscopic microfracture vs. arthroscopic autologous matrix-induced chondrogenesis for the treatment of articular cartilage defects of the talus.Knee Surg Sports Traumatol Arthrosc. 2019 Sep;27(9):2731-2736. doi: 10.1007/s00167-018-5278-7. Epub 2018 Nov 3. Knee Surg Sports Traumatol Arthrosc. 2019. PMID: 30392029
-
Is there clinical evidence to support autologous matrix-induced chondrogenesis (AMIC) for chondral defects in the talus? A systematic review and meta-analysis.Foot Ankle Surg. 2021 Apr;27(3):236-245. doi: 10.1016/j.fas.2020.07.011. Epub 2020 Aug 16. Foot Ankle Surg. 2021. PMID: 32811744
-
The efficacy of autologous matrix-induced chondrogenesis (AMIC) for osteochondral lesions of the talus in the mid-long term: a systematic review and meta-analysis.J Orthop Surg Res. 2024 Jun 24;19(1):373. doi: 10.1186/s13018-024-04864-z. J Orthop Surg Res. 2024. PMID: 38915104 Free PMC article.
References
-
- Kreuz PC, Steinwachs M, Erggelet C, Lahm A, Henle P, Niemeyer P. Mosaicplasty with autogenous talar autograft for osteochondral lesions of the talus after failed primary arthroscopic management: a prospective study with a 4-year follow-up. Am J Sports Med. 2006;34(1):55 63. (10.1177/0363546505278299) - DOI - PubMed
-
- Bruns J, Behrens P. Osteochondrosis dissecans. Arthroskopie. 1998;11(4):166 176.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
