

Role of molecular alterations in transplantation decisions for patients with primary myelofibrosis
- PMID: 39561372
- PMCID: PMC11869958
- DOI: 10.1182/bloodadvances.2024014368
Role of molecular alterations in transplantation decisions for patients with primary myelofibrosis
Abstract
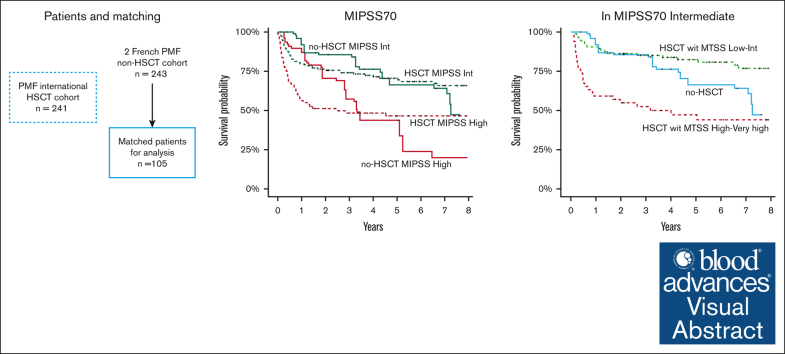
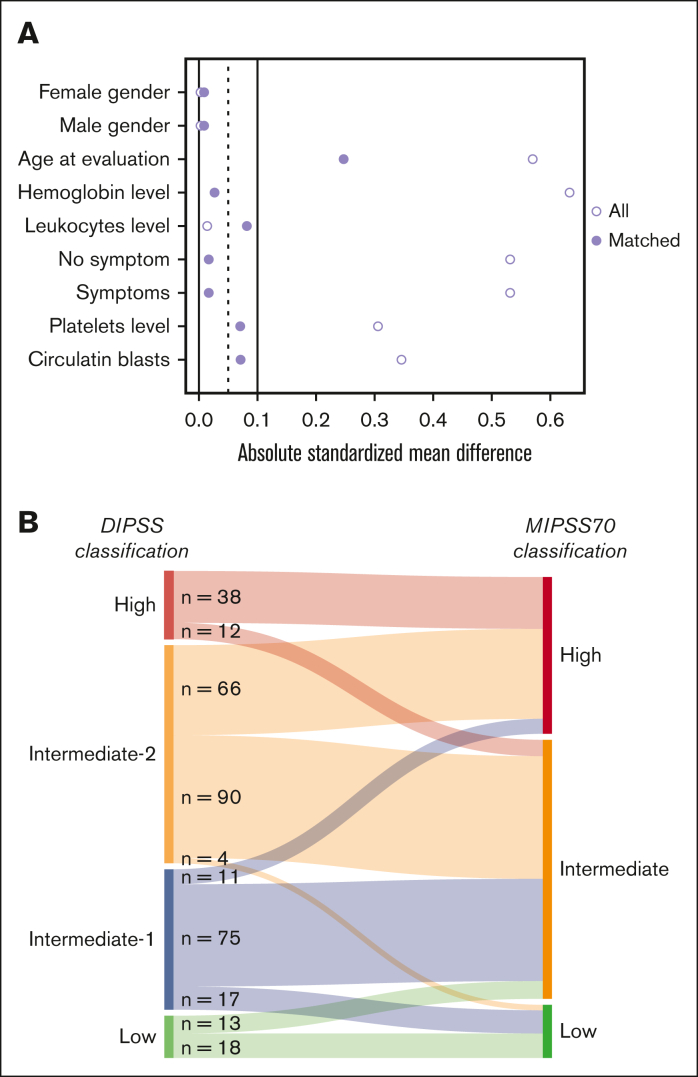
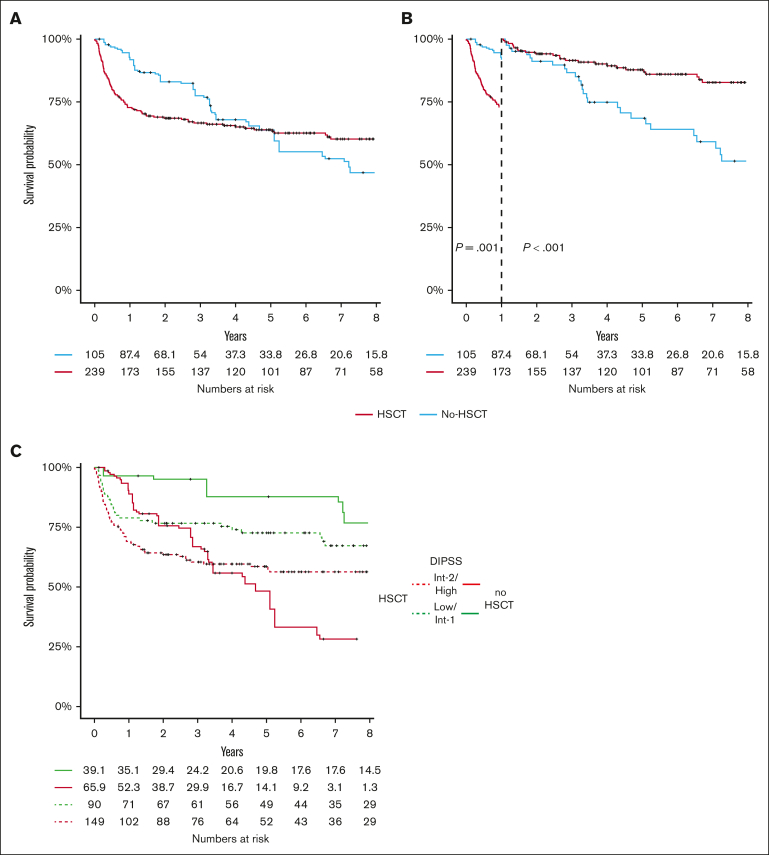
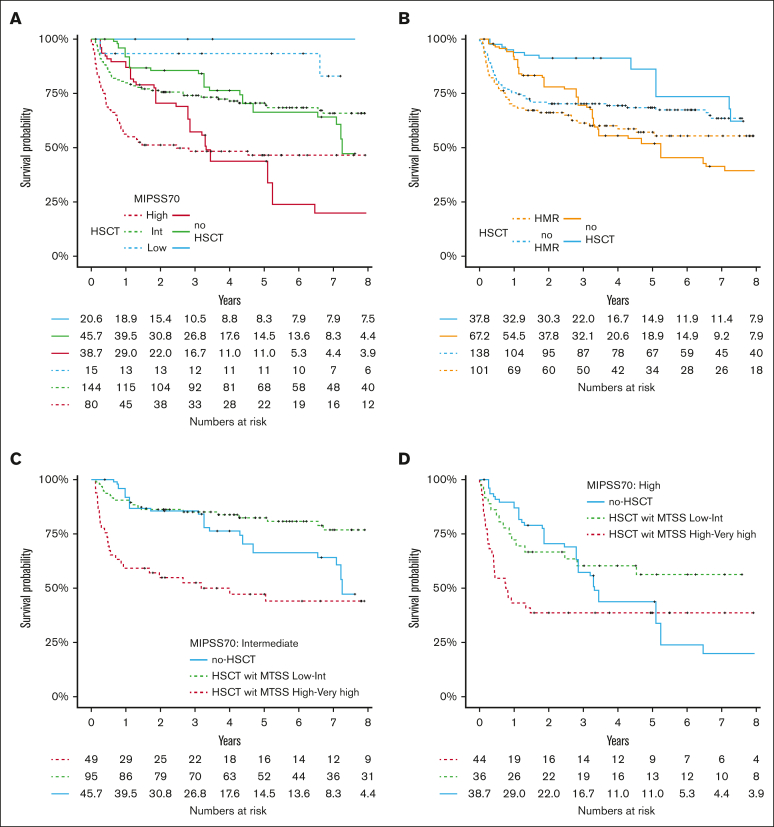
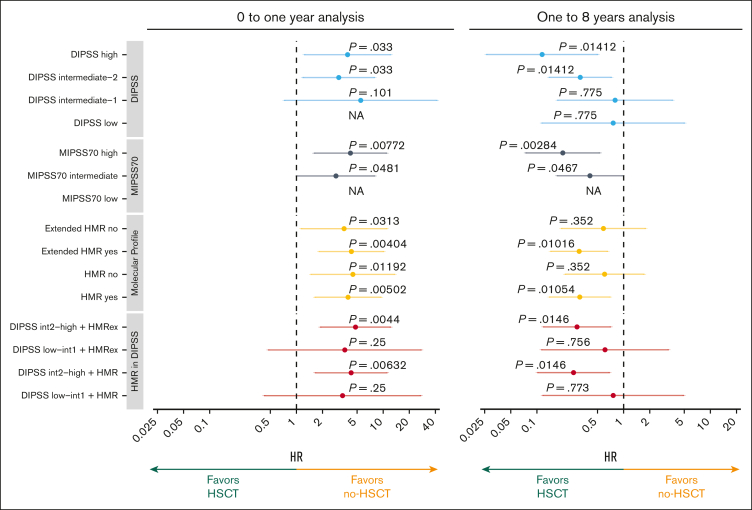
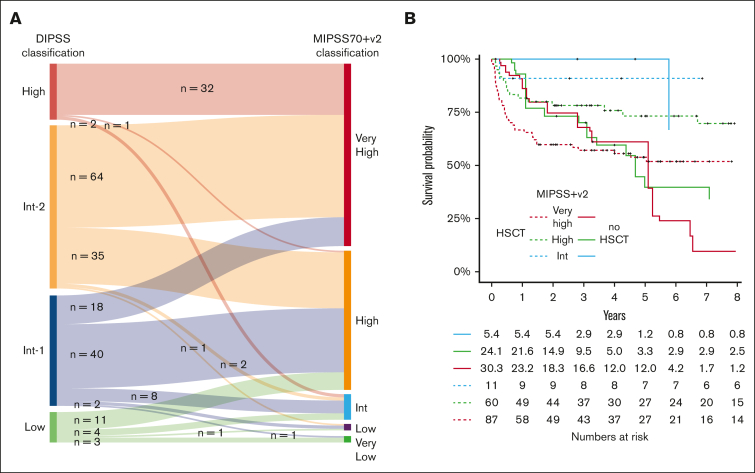
The aim of our study was to analyze the potential survival benefit associated with hematopoietic stem cell transplantation (HSCT) according to clinicobiological scores, which incorporate mutation-enhanced international prognostic score system (MIPSS) to facilitate decision-making in this context. One transplant (n = 241) and 1 nontransplant cohort (n = 239) were used to test the hypothesis that patients with primary myelofibrosis with higher risk molecular score benefit from HSCT. A weighted propensity score was applied to balance confounding factors with the transplanted cohort as reference. Weighted Cox proportional hazard models and logistic regression analyses were performed. Overall, 105 patients who did not receive transplant could be matched to the 239 patients who did receive transplants. HSCT was associated with a higher 6-year overall survival rate in intermediate-2 (60.1% vs 41.5%) and high-risk DIPSS patients (44.4% vs 6.55%), high-risk MIPSS70 (46.5% vs 23.9%), high-risk (73.2% vs 39.7%) or very high-risk MIPSS70+V2 (51.8% vs 24%). Patients with intermediate MIPSS70 scores have an advantage of survival with HSCT only when their myelofibrosis transplant scoring system (MTSS) were low or intermediate. Patients who received transplant had an increased mortality risk the first year, but a significant benefit with HSCT after the 1-year landmark was observed in higher risk patients. This study confirms that, similar to DIPSS, MIPSS70 and MIPSS70+V2 risk score in addition to MTSS can be used to determine which patients with primary myelofibrosis have survival benefit from HSCT over non-HSCT strategies.
© 2025 American Society of Hematology. Published by Elsevier Inc. Licensed under Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International (CC BY-NC-ND 4.0), permitting only noncommercial, nonderivative use with attribution. All other rights reserved.
Conflict of interest statement
Conflict-of-interest disclosure: The authors declare no competing financial interests.
Figures
References
-
- Passamonti F, Cervantes F, Vannucchi AM, et al. Dynamic International Prognostic Scoring System (DIPSS) predicts progression to acute myeloid leukemia in primary myelofibrosis. Blood. 2010;116(15):2857–2858. - PubMed
-
- Gangat N, Caramazza D, Vaidya R, et al. DIPSS plus: a refined Dynamic International Prognostic Scoring System for primary yelofibrosis that incorporates prognostic information from karyotype, platelet count, and transfusion status. J Clin Orthod. 2011;29(4):392–397. - PubMed
-
- Guglielmelli P, Lasho TL, Rotunno G, et al. MIPSS70: Mutation-Enhanced International Prognostic Score System for transplantation-age patients with primary myelofibrosis. J Clin Oncol. 2018;36(4):310–318. - PubMed
-
- Tefferi A, Guglielmelli P, Lasho TL, et al. MIPSS70+ version 2.0: mutation and karyotype-enhanced international prognostic scoring system for primary myelofibrosis. J Clin Oncol. 2018;36(17):1769–1770. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
