

Basilar invagination and atlantoaxial dislocation as a complication of severe dystrophic cervical kyphosis correction in neurofibromatosis type 1: Report of a rare case and review of literature
- PMID: 39561572
- PMCID: PMC11615887
- DOI: 10.1016/j.ijscr.2024.110599
Basilar invagination and atlantoaxial dislocation as a complication of severe dystrophic cervical kyphosis correction in neurofibromatosis type 1: Report of a rare case and review of literature
Abstract
Introduction and importance: Neurofibromatosis type 1 (NF1) affects the musculoskeletal system as well as the cervical spine. It is associated with severe, progressive cervical kyphosis. Surgical intervention is the treatment of choice to avoid neurological impairment and malalignment.
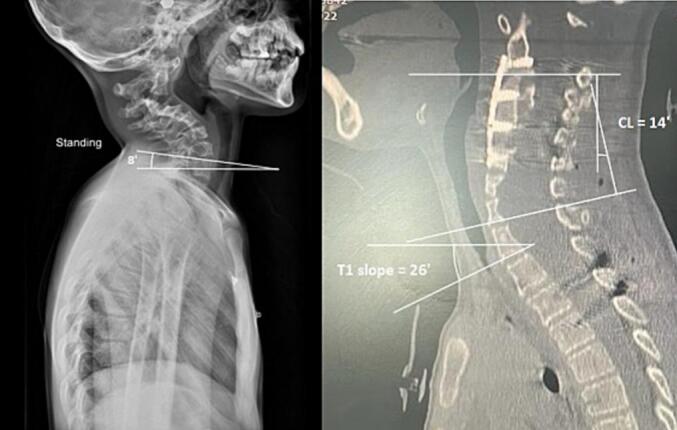
Case presentation: We herein report an 11-year-old NF-1 patient with severe cervical kyphosis and intact neurological status. We applied five days of cervical traction followed by surgery utilizing the combined cervical approach (posterior release, anterior corpectomy and reconstruction, and posterior cervicothoracic instrumentation). In one-year follow-up, atlantoaxial dislocation (AAD) and basilar invagination (BI) were detected in neuroimagings. The complication was corrected by adding C1 to the previous construct via unilateral C1 lateral mass screw, contralateral C1 sublaminar hook, unilateral C3 and contralateral C4 sublaminar hook insertion, fixed with contoured rods medial to previous rods. This led to the correction of the AAD and the BI and the patients remained neurologically intact.
Clinical discussion: Severe cervical kyphosis in the setting of NF-1 is progressive and carries a considerable risk of neurologic compromise. Surgical intervention is thus necessary.
Conclusion: The combined approach with complete spinal column reconstruction is the surgical approach of choice. However, complete curve correction to near-normal lordosis carries the risk of proximal junctional failure (PJF).
Keywords: Atlantoaxial dislocation; Basilar invagination; Cervical kyphosis; Neurofibromatosis-1; Proximal junctional failure.
Copyright © 2024 The Authors. Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
Declaration of competing interest None of the authors have any conflict of interest to declare regarding the manuscript.
Figures







References
-
- Curtis-Lopez C.M., Soh C., Ealing J., Gareth Evans D., Burkitt Wright E.M.M., Vassallo G., et al. Clinical and neuroradiological characterisation of spinal lesions in adults with neurofibromatosis type 1. J. Clin. Neurosci. 2020;77:98–105. - PubMed
-
- Pillai S.S., Ramsheela P. Spinal deformities in neurofibromatosis 1. J. Orthop. Assoc. South Indian States. 2020;17(2):49.
-
- Lee S.H., Son E.S., Seo E.M., Suk K.S., Kim K.T. Factors determining cervical spine sagittal balance in asymptomatic adults: correlation with spinopelvic balance and thoracic inlet alignment. Spine J. 2015;15(4):705–712. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
