

Atrial fibrillation nomenclature, definitions, and mechanisms: Position paper from the international Working Group of the Signal Summit
- PMID: 39561931
- PMCID: PMC12084426
- DOI: 10.1016/j.hrthm.2024.11.012
Atrial fibrillation nomenclature, definitions, and mechanisms: Position paper from the international Working Group of the Signal Summit
Abstract
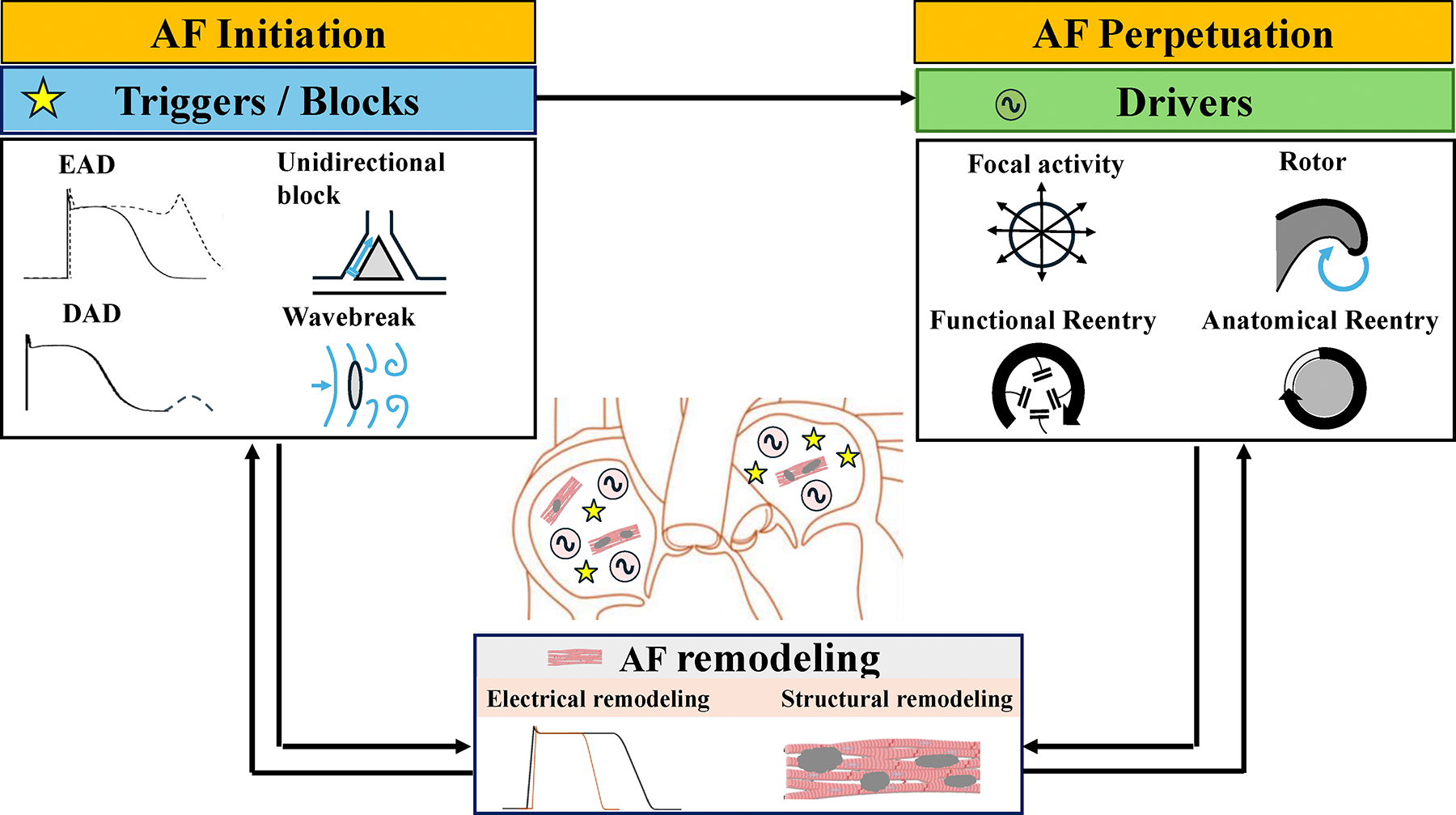
The international Working Group of the Signal Summit is a consortium of experts in the field of cardiac electrophysiology dedicated to advancing knowledge on understanding and clinical application of signal recording and processing techniques. In 2023, the working group met in Reykjavik, Iceland, and laid the foundation for this manuscript. Atrial fibrillation (AF) is the most common arrhythmia in adults, with a rapidly increasing prevalence worldwide. Despite substantial research efforts, advancements in elucidating the underlying mechanisms of AF have been relatively modest. Since the discovery of pulmonary veins as a frequent trigger region for AF initiation more than 2½ decades ago, advancements in patient care have primarily focused on technologic innovations to improve the safety and efficacy of pulmonary vein isolation (PVI). Several factors may explain the limited scientific progress made. First, whereas AF initiation usually begins with an ectopic beat, the mechanisms of initiation, maintenance, and electrical propagation have not been fully elucidated in humans, largely owing to suboptimal spatiotemporal mapping. Second, underlying structural changes have not been clarified and may involve different types of reentry. Third, inconsistent definitions and terminology regarding fibrillatory characteristics contribute to the challenges of comparing results between studies. Fourth, a growing appreciation for phenotypical differences probably explains the wide range of clinical outcomes to catheter ablation in patients with seemingly similar AF types. Last, restoring sinus rhythm in advanced phenotypic forms of AF is often not feasible or may require extensive ablation with minimal or no positive impact on quality of life. The aims of this international position paper are to provide practical definitions as a foundation for discussing potential mechanisms and mapping results and to propose pathways toward meaningful advancements in AF research, ultimately leading to improved therapies for AF.
Keywords: Ablation; Atrial fibrillation; Definitions; Mapping; Mechanisms; Treatment.
Copyright © 2024 Heart Rhythm Society. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Disclosures The authors have no conflicts of interest to disclose.
Figures
Similar articles
-
Curative catheter ablation in atrial fibrillation and typical atrial flutter: systematic review and economic evaluation.Health Technol Assess. 2008 Nov;12(34):iii-iv, xi-xiii, 1-198. doi: 10.3310/hta12340. Health Technol Assess. 2008. PMID: 19036232
-
The Black Book of Psychotropic Dosing and Monitoring.Psychopharmacol Bull. 2024 Jul 8;54(3):8-59. Psychopharmacol Bull. 2024. PMID: 38993656 Free PMC article. Review.
-
Mechanistic Insights From Trials of Atrial Fibrillation Ablation: Charting a Course for the Future.Circ Arrhythm Electrophysiol. 2024 Aug;17(8):e012939. doi: 10.1161/CIRCEP.124.012939. Epub 2024 Jul 23. Circ Arrhythm Electrophysiol. 2024. PMID: 39041221 Free PMC article. Review.
-
Catheter ablation for paroxysmal and persistent atrial fibrillation.Cochrane Database Syst Rev. 2012 Apr 18;2012(4):CD007101. doi: 10.1002/14651858.CD007101.pub2. Cochrane Database Syst Rev. 2012. PMID: 22513945 Free PMC article.
-
Intravenous magnesium sulphate and sotalol for prevention of atrial fibrillation after coronary artery bypass surgery: a systematic review and economic evaluation.Health Technol Assess. 2008 Jun;12(28):iii-iv, ix-95. doi: 10.3310/hta12280. Health Technol Assess. 2008. PMID: 18547499
Cited by
-
Advancing Atrial Fibrillation Research: The Role of Animal Models, Emerging Technologies and Translational Challenges.Biomedicines. 2025 Jan 27;13(2):307. doi: 10.3390/biomedicines13020307. Biomedicines. 2025. PMID: 40002720 Free PMC article. Review.
-
IL-11 promotes Ang II-induced autophagy inhibition and mitochondrial dysfunction in atrial fibroblasts.Open Life Sci. 2025 Mar 11;20(1):20251063. doi: 10.1515/biol-2025-1063. eCollection 2025. Open Life Sci. 2025. PMID: 40092733 Free PMC article.
References
-
- Haissaguerre M, Jais P, Shah DC, Takahashi A, Hocini M, Quiniou G, Garrigue S, Le Mouroux A, Le Metayer P, Clementy J. Spontaneous initiation of atrial fibrillation by ectopic beats originating in the pulmonary veins. N Engl J Med 1998;339:659–666. - PubMed
-
- Clarnette JA, Brooks AG, Mahajan R, Elliott AD, Twomey DJ, Pathak RK, Kumar S, Munawar DA, Young GD, Kalman JM, Lau DH, Sanders P. Outcomes of persistent and long-standing persistent atrial fibrillation ablation: a systematic review and meta-analysis. Europace 2018;20:f366–f376. - PubMed
-
- Kottkamp H, Tanner H, Kobza R, Schirdewahn P, Dorszewski A, Gerds-Li JH, Carbucicchio C, Piorkowski C, Hindricks G. Time courses and quantitative analysis of atrial fibrillation episode number and duration after circular plus linear left atrial lesions: trigger elimination or substrate modification: early or delayed cure? J Am Coll Cardiol 2004;44:869–877. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
