

Brain tissue microstructure in a prospective, longitudinal, population-based cohort of preterm and term-born young adults
- PMID: 39561978
- PMCID: PMC12018296
- DOI: 10.1111/jcpp.14069
Brain tissue microstructure in a prospective, longitudinal, population-based cohort of preterm and term-born young adults
Abstract
Background: Fifteen million infants annually are born prematurely, placing them at high risk for life-long adverse neurodevelopmental outcomes. Whether brain tissue abnormalities that accompany preterm birth persist into young adulthood and are associated with long-term cognitive or psychiatric outcomes is not known.
Methods: From infancy into young adulthood, we followed a population-based sample of consecutively identified preterm infants and their matched term controls. The preterm group was born at an average gestational age of 31.5 ± 2.6 weeks. We obtained Diffusion Tensor Imaging scans and assessed cognitive and psychiatric outcomes in young adulthood, at a mean age of 19 (range 17.6-20.8) years. Usable data were acquired from 180 participants (89 preterm, 91 term).
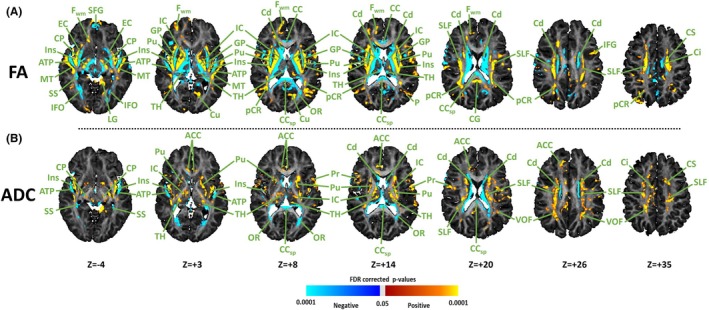
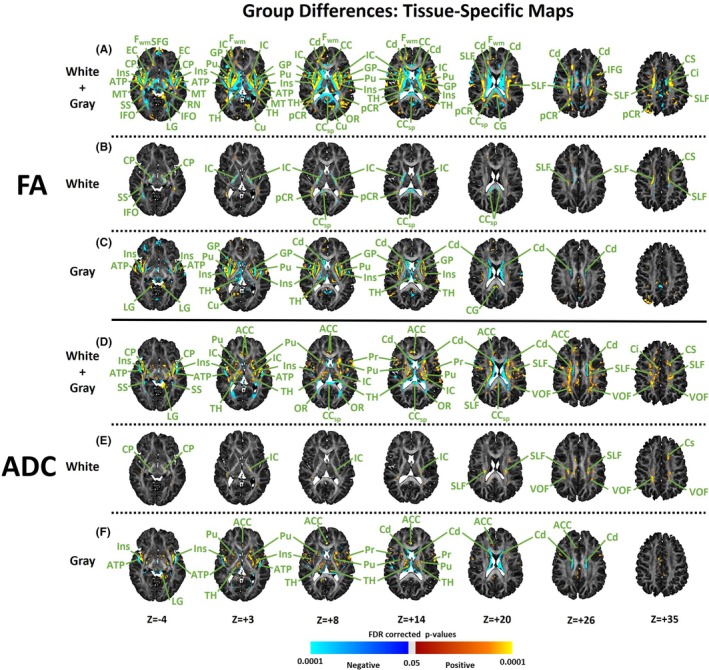
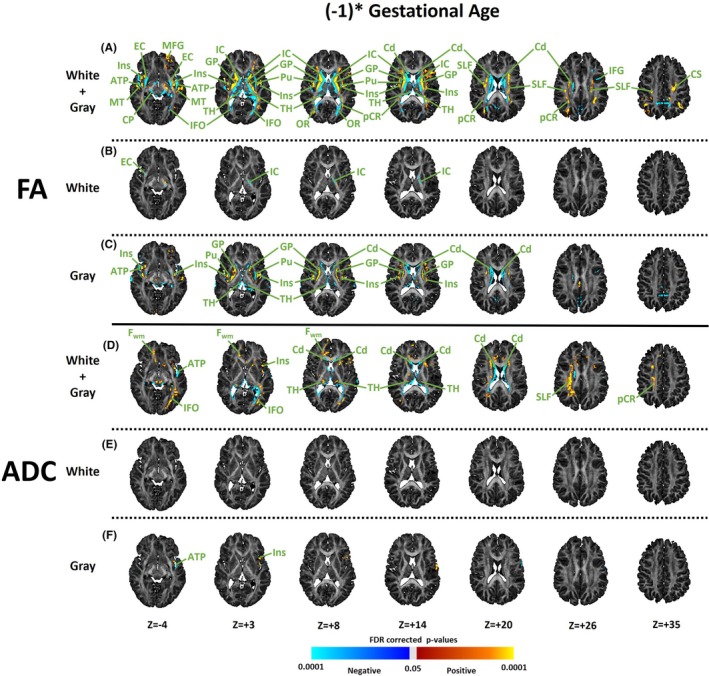
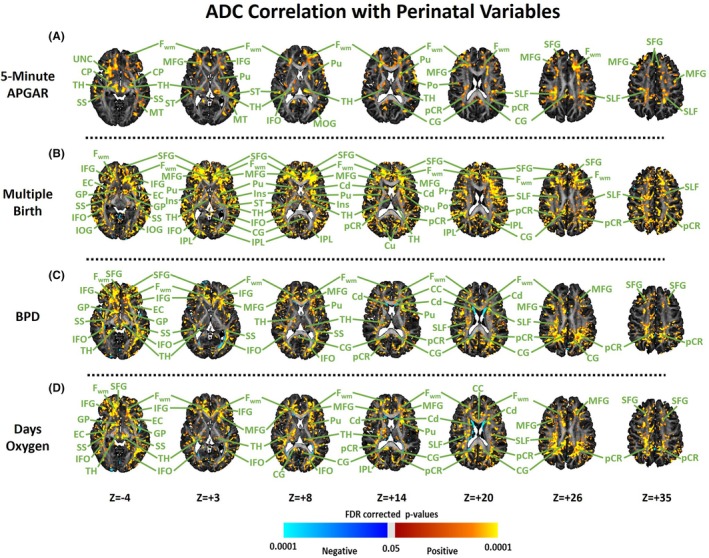
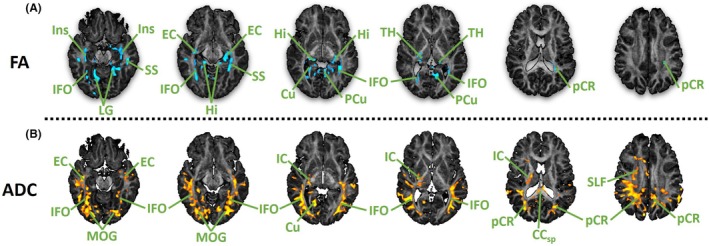
Results: Preterm birth was associated with lower fractional anisotropy (FA) and higher average diffusion coefficient (ADC) values in deep white matter tracts of the internal capsule, cerebral peduncles, inferior frontal-occipital fasciculus, sagittal stratum and splenium of the corpus callosum, as well as in grey matter of the caudate, putamen and thalamus. A younger gestational age at birth accentuated these tissue abnormalities. Perinatal characteristics, including lower 5-min APGAR score, history of bronchopulmonary dysplasia, more days of oxygen supplementation and multiple births all increased ADC values in deep white matter tracts and grey matter throughout the brain. Preterm individuals had significantly lower full-scale IQ and more frequent lifetime psychiatric disorders. Those with psychiatric illnesses had significantly higher ADC and lower FA values throughout the deep posterior white matter.
Conclusions: Abnormalities in brain tissue microstructure associated with preterm birth persist into young adulthood and likely represent disordered myelination and accompanying axonal pathology. These disturbances are associated with a higher likelihood of developing a psychiatric disorder by young adulthood. Brain tissue disturbances were accentuated in those born at younger gestational ages and in those with a history of perinatal complications associated with infection and inflammation.
Keywords: Premature birth; diffusion tensor imaging; magnetic resonance imaging; preterm birth.
© 2024 The Author(s). Journal of Child Psychology and Psychiatry published by John Wiley & Sons Ltd on behalf of Association for Child and Adolescent Mental Health.
Figures
References
-
- Abhinav, K. , Yeh, F.C. , Pathak, S. , Suski, V. , Lacomis, D. , Friedlander, R.M. , & Fernandez‐Miranda, J.C. (2014). Advanced diffusion MRI fiber tracking in neurosurgical and neurodegenerative disorders and neuroanatomical studies: A review. Biochimica et Biophysica Acta‐Molecular Basis of Disease, 1842, 2286–2297. - PubMed
-
- Alexander, A.L. , Hasan, K.M. , Lazar, M. , Tsuruda, J.S. , & Parker, D.L. (2001). Analysis of partial volume effects in diffusion‐tensor MRI. Magnetic Resonance in Medicine: An Official Journal of the International Society for Magnetic Resonance in Medicine, 45, 770–780. - PubMed
-
- Alexandrou, G. , Mårtensson, G. , Skiöld, B. , Blennow, M. , Adén, U. , & Vollmer, B. (2014). White matter microstructure is influenced by extremely preterm birth and neonatal respiratory factors. Acta Paediatrica, 103, 48–56. - PubMed
-
- Assaf, Y. , & Basser, P.J. (2005). Composite hindered and restricted model of diffusion (CHARMED) MR imaging of the human brain. NeuroImage, 27, 48–58. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
