

Prognostic significance of mutation type and chromosome fragility in Fanconi anemia
- PMID: 39562502
- PMCID: PMC11705201
- DOI: 10.1002/ajh.27520
Prognostic significance of mutation type and chromosome fragility in Fanconi anemia
Abstract
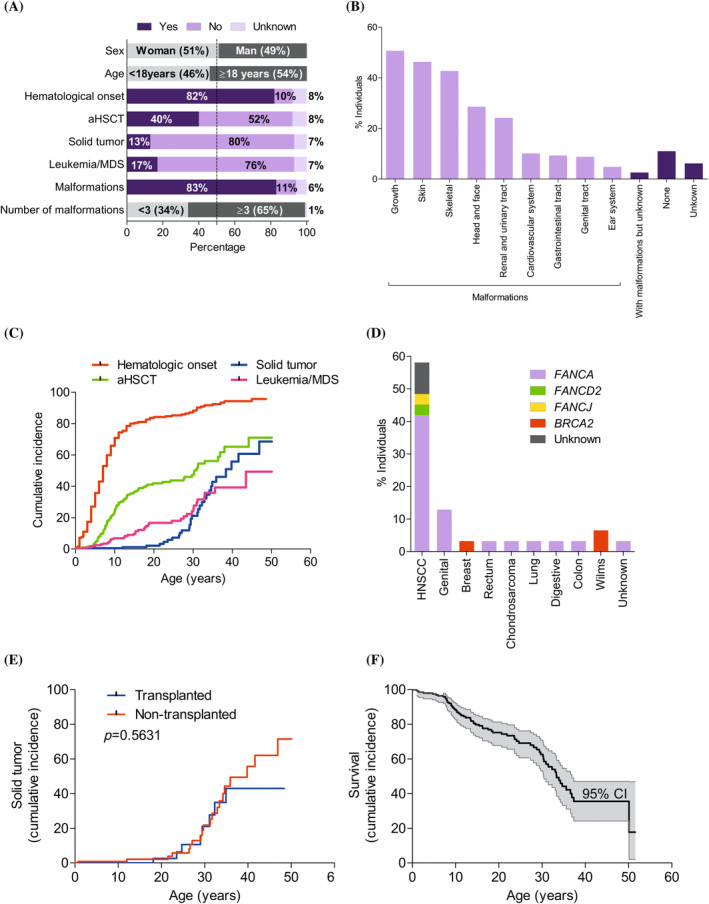
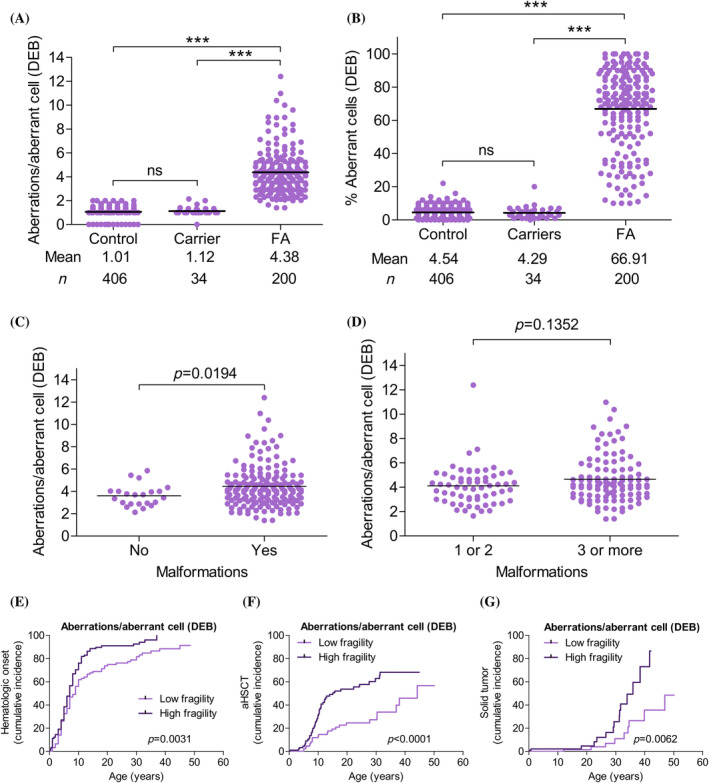
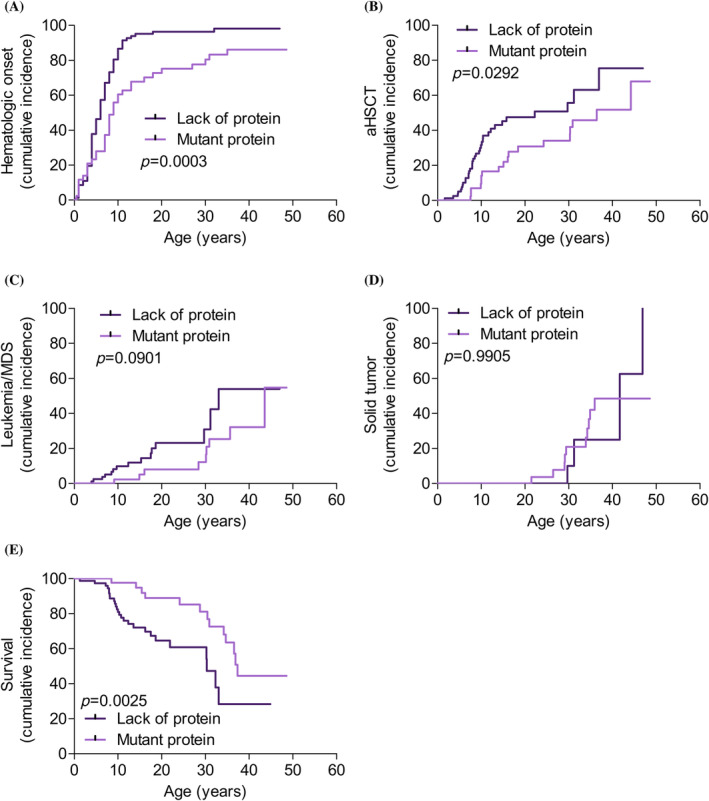
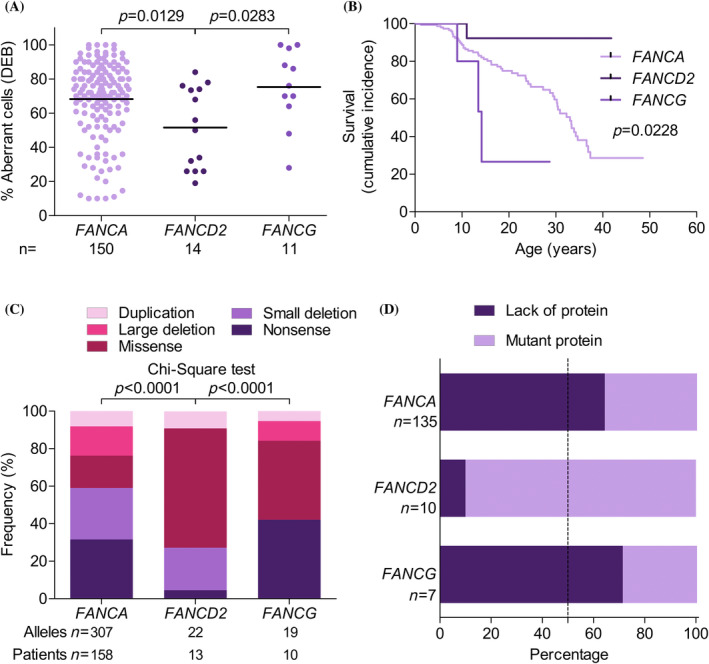
Fanconi anemia (FA) is a rare genetic disease characterized by high phenotypic and genotypic heterogeneity, and extreme chromosome fragility. To better understand the natural history of FA, identify genetic risk and prognostic factors, and develop novel therapeutic strategies, the Spanish Registry of Patients with FA collects data on clinical features, chromosome fragility, genetic subtypes, and DNA sequencing with informed consent of participating individuals. In this article, we describe the clinical evolution of 227 patients followed up for up to 30 years, for whom our data indicate a cumulative cancer incidence of 86% by age 50. We found that patients with lower chromosome fragility had a milder malformation spectrum and better outcomes in terms of later-onset hematologic impairment, less severe bone marrow failure, and lower cancer risk. We also found that outcomes were better for patients with mutations leading to mutant FANCA protein expression (genetic hypomorphism) than for patients lacking this protein. Likewise, prognosis was consistently better for patients with biallelic mutations in FANCD2 (mainly hypomorphic mutations) than for patients with biallelic mutations in FANCA and FANCG, with the lack of the mutant protein in patients with biallelic mutations in FANCG contributing to their poorer outcomes. Our results regarding the clinical impact of chromosome fragility and genetic hypomorphism suggest that mutant FA proteins retain residual activity. This finding should encourage the development of novel therapeutic strategies aimed at partially or fully enhancing mutant FA function, thereby preventing or delaying bone marrow failure and cancer in patients with FA. Clinical Trial Registration number: NCT06490510.
© 2024 The Author(s). American Journal of Hematology published by Wiley Periodicals LLC.
Conflict of interest statement
J.S. has signed agreements in the last 3 years (advisory boards, service provision, research collaboration, or material transfer) with Boehringer Ingelheim, Glaxo Smith Kline, Moderna Therapeutics, Roche, Rocket Pharmaceuticals and Pfizer.
P.R., S.N., and J.A.B. receive funding and have licensed the PGK‐FANCA‐WPRE* lentiviral vector to Rocket Pharmaceuticals Ltd., and P.R., S.N., and J.A.B. are inventors on patents filed by CIEMAT, CIBERER, and Fundación Jiménez Díaz, and may be entitled to receive financial benefits from the licensing of such patents. J.A.B is a consultant to Rocket Pharmaceuticals.
J.A.B. receives honorariums as a consultant, holds stock options and has received funding for research on gene therapy from Rocket Pharmaceuticals. Cofounder of KiJi Therapeutics.
All the other authors declare that they have no conflict of interest.
Figures
References
-
- Orphanet . Orphanet. 2023. https://www.orpha.net/
-
- Kuehl J, Pickel S, Xue Y, Zhang Y, Wang W, Schindler D. Biallelic mutations in FAAP100 predispose to Fanconi anemia (FA). Fanconi Anemia Research Fundation Scientific Symposium (p. 26). 2018.
-
- Meetei AR, Levitus M, Xue Y, et al. X‐linked inheritance of Fanconi anemia complementation group B. Nat Genet. 2004;36(11):1219‐1224. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
- ICREA-Academia program/Fundació Institut Català de Recerca i Estudis Avançats
- FABRAT PID2021-122411OB-I00/AEI/10.13039/50110001/Ministerio de Ciencia, Innovación y Universidades
- 2021-SGR-00835/Agència de Gestió d'Ajuts Universitaris i de Recerca
- ICI22/00076/the Instituto de Salud Carlos III (ISCIII) and fondos Next Generation EU
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
