

Efficacy of the maxillary anterior segmental distraction osteogenesis in patients with cleft lip and palate
- PMID: 39563318
- PMCID: PMC11575218
- DOI: 10.1186/s12903-024-05208-3
Efficacy of the maxillary anterior segmental distraction osteogenesis in patients with cleft lip and palate
Abstract
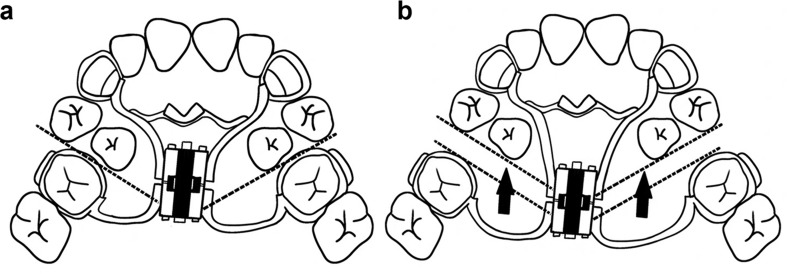
Background: Cleft lip and palate (CLP) is one of the most common birth defects worldwide. It typically results in significant maxillary dysplasia, causing severe oral function problems and substantially affecting the patient's facial aesthetics. Maxillary anterior segmental distraction osteogenesis (MASDO) has gained popularity in recent years as an effective treatment for correcting maxillary dysplasia. However, the evaluation of its effectiveness in patients with CLP varies across different studies. Our research was aimed at providing evidence of the effects of MASDO among CLP patients.
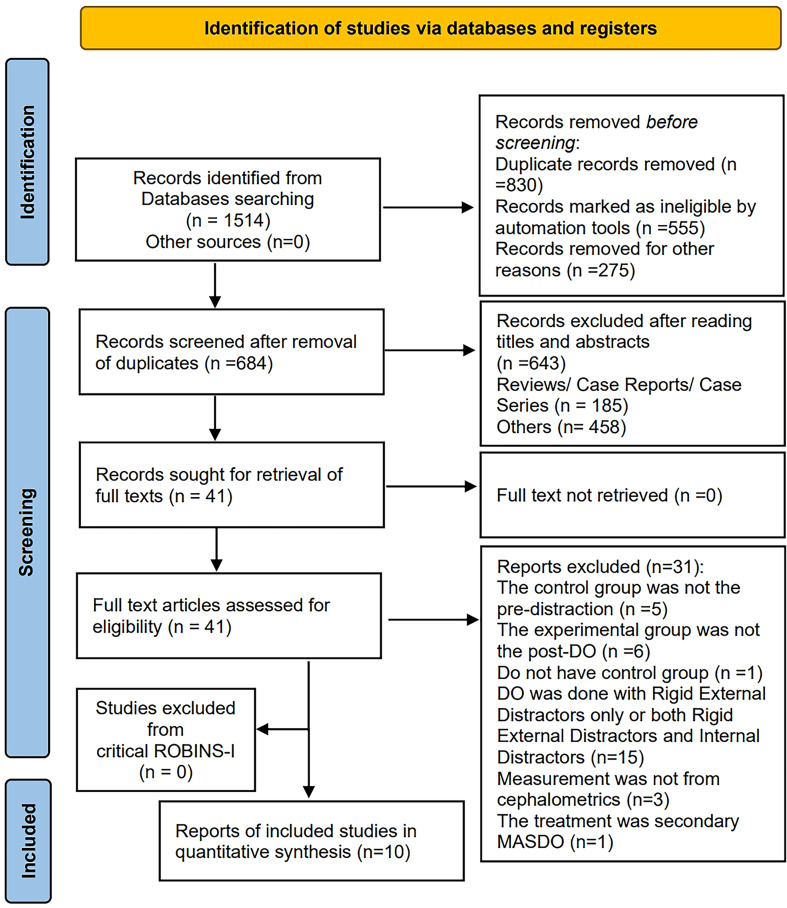
Methods: A meta-analysis covered Medline, Web of Science, Embase, Scopus, and Cochrane Library. Controlled clinical trial studies published before February 2024 and analyzed changes in maxillary cephalometric landmarks before and after MASDO among patients with maxillary hypoplasia and CLP were included.
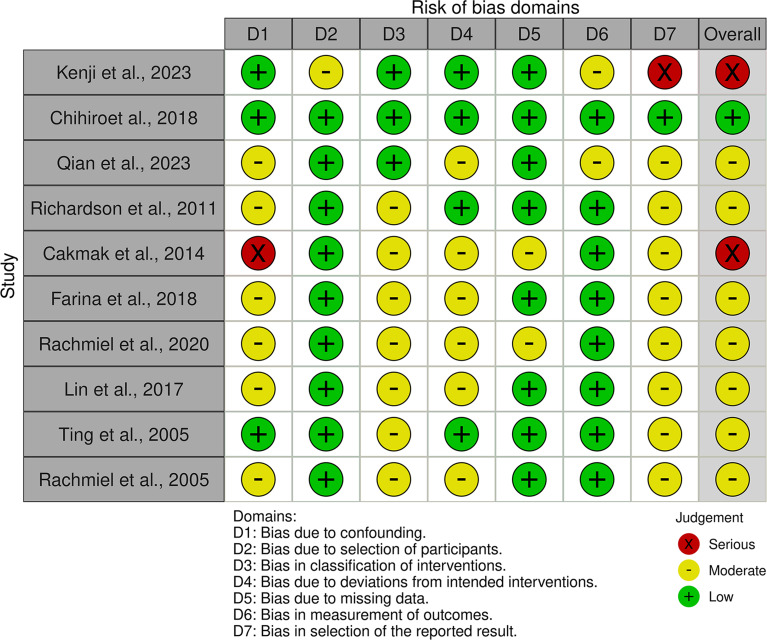
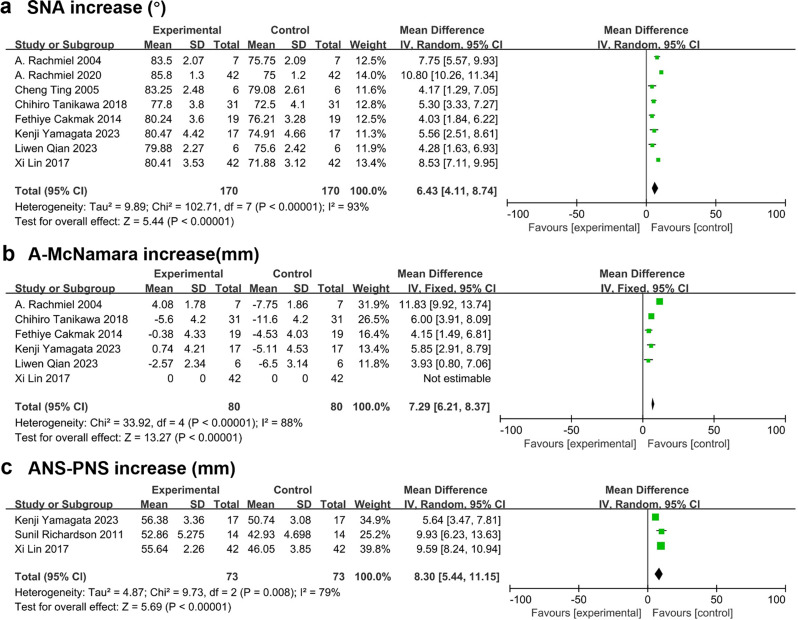
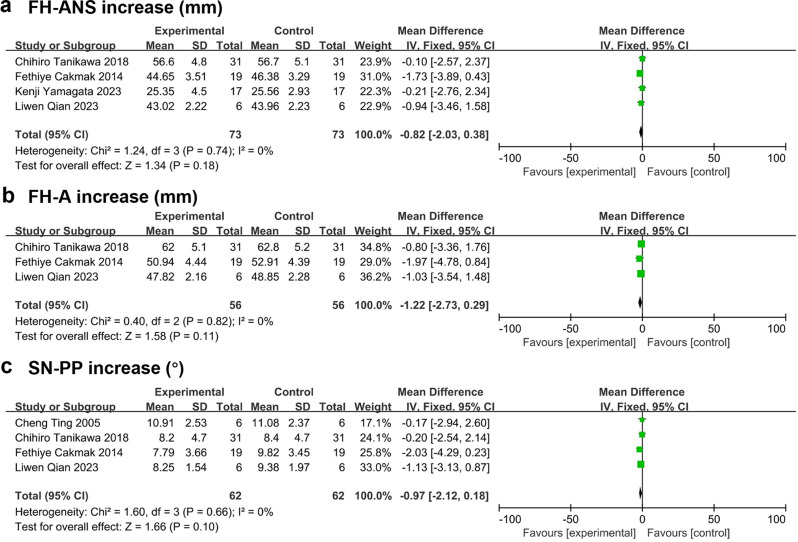
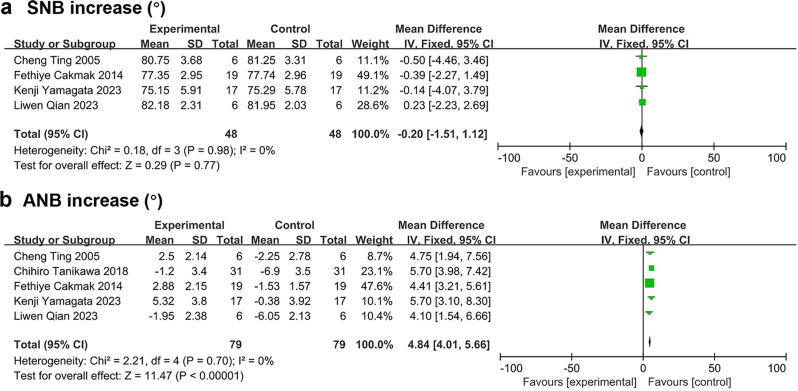
Results: Our meta-analysis included 10 papers in total. One study was at low risk of bias, seven were at medium risk, and two were at serious risk. MASDO significantly increased the maxillary length. The mean SNA angle increased by 6.43° (95% CI, 4.11° to 8.74°) and A-McNamara rose by 7.29 mm (95% CI, 6.21 mm to 8.37 mm). The maxilla also showed a slight counterclockwise rotation; however, this reached no statistical significance. The mandibular position did not vary remarkably. Moreover, a significant increase in upper anterior tooth tipping and overjet, a decrease in overbite, and an improvement in nasolabial soft tissue were observed.
Conclusions: MASDO might be a valid therapy option for CLP patients. It causes a significant increase in the maxillary length, anterior tooth crossbite, and nasolabial soft tissue were also greatly improved.
Keywords: Cleft lip and palate; Maxillary hypoplasia; Meta-analysis; Systematic review.
© 2024. The Author(s).
Conflict of interest statement
Figures

Similar articles
-
Efficacy of Maxillary Anterior Segmental Distraction Osteogenesis in Patients With Cleft Lip and Palate.Cleft Palate Craniofac J. 2018 Nov;55(10):1375-1381. doi: 10.1177/1055665618758692. Epub 2018 Mar 13. Cleft Palate Craniofac J. 2018. PMID: 29533696
-
Maxillary anterior segmental distraction osteogenesis to correct maxillary hypoplasia and dental crowding in cleft palate patients: a preliminary study.BMC Oral Health. 2023 May 24;23(1):321. doi: 10.1186/s12903-023-03038-3. BMC Oral Health. 2023. PMID: 37226215 Free PMC article.
-
Advancement of maxillary anterior segment by distraction osteogenesis for severe maxillary retrusion in cleft lip and palate.Chin Med J (Engl). 2014;127(3):500-5. Chin Med J (Engl). 2014. PMID: 24451957
-
Effects of anterior maxillary distraction compared to LeFort-1 osteotomy and total maxillary distraction osteogenesis for treating hypoplastic maxilla in patients with cleft lip and palate- A systematic review and meta-analysis.J Stomatol Oral Maxillofac Surg. 2023 Feb;124(1S):101308. doi: 10.1016/j.jormas.2022.10.007. Epub 2022 Oct 8. J Stomatol Oral Maxillofac Surg. 2023. PMID: 36220549
-
Maxillary distraction osteogenesis versus orthognathic surgery for cleft lip and palate patients.Cochrane Database Syst Rev. 2018 Aug 10;8(8):CD010403. doi: 10.1002/14651858.CD010403.pub3. Cochrane Database Syst Rev. 2018. PMID: 30095853 Free PMC article.
Cited by
-
Successful interdisciplinary retreatment after initial treatment failure in a cleft lip adolescent.BMC Oral Health. 2025 May 1;25(1):675. doi: 10.1186/s12903-025-06055-6. BMC Oral Health. 2025. PMID: 40312655 Free PMC article.
References
-
- Tan CS, Hariri F, Hassan MK. Severe midface and Maxillary Hypoplasia in Non-cleft and non-syndromic patients: a 2-Stage Surgical Strategy using distraction osteogenesis and orthognathic surgery. J STOMATOL ORAL MAXI. 2023;101552. 10.1016/j.jormas.2023.101552. - PubMed
-
- Wang Y, Li J, Xu Y, Huang N, Shi B, Li J. Accuracy of virtual Surgical planning-assisted management for Maxillary Hypoplasia in Adult patients with cleft lip and palate. J PLAST RECONSTR AES. 2020;73:134–40. 10.1016/j.bjps.2019.07.003. - PubMed
-
- Lou Q, Wang X, Chen Y. Speech outcomes Comparison between Adult Velopharyngeal Insufficiency and patients with Unrepaired Cleft Palate. J CRANIOFAC SURG. 2021;32:655–9. 10.1097/SCS.0000000000006994. - PubMed
-
- Crepaldi TA, Vitor L, Carrara C, Rios D, Cruvinel T, Almeida A, Soares S, Machado M, Oliveira TM. Do cleft lip and palate types affect Health-Related Quality of Life of adolescents? J CRANIOFAC SURG. 2019;30:829–33. 10.1097/SCS.0000000000005175. - PubMed
-
- Wangsrimongkol B, Flores RL, Staffenberg DA, Rodriguez ED, Shetye PR, PALATE-CRAN J. 2022; 59:98–109. 10.1177/1055665621996108 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
