

Central venous catheter-related infections: a systematic review, meta-analysis, trial sequential analysis and meta-regression comparing ultrasound guidance and landmark technique for insertion
- PMID: 39563416
- PMCID: PMC11577744
- DOI: 10.1186/s13054-024-05162-0
Central venous catheter-related infections: a systematic review, meta-analysis, trial sequential analysis and meta-regression comparing ultrasound guidance and landmark technique for insertion
Abstract
Background: During central venous catheterization (CVC), ultrasound (US) guidance has been shown to reduce mechanical complications and increase success rates compared to the anatomical landmark (AL) technique. However, the impact of US guidance on catheter-related infections remains controversial. This systematic review and meta-analysis aimed to compare the risk of catheter-related infection with US-guided CVC versus AL technique.
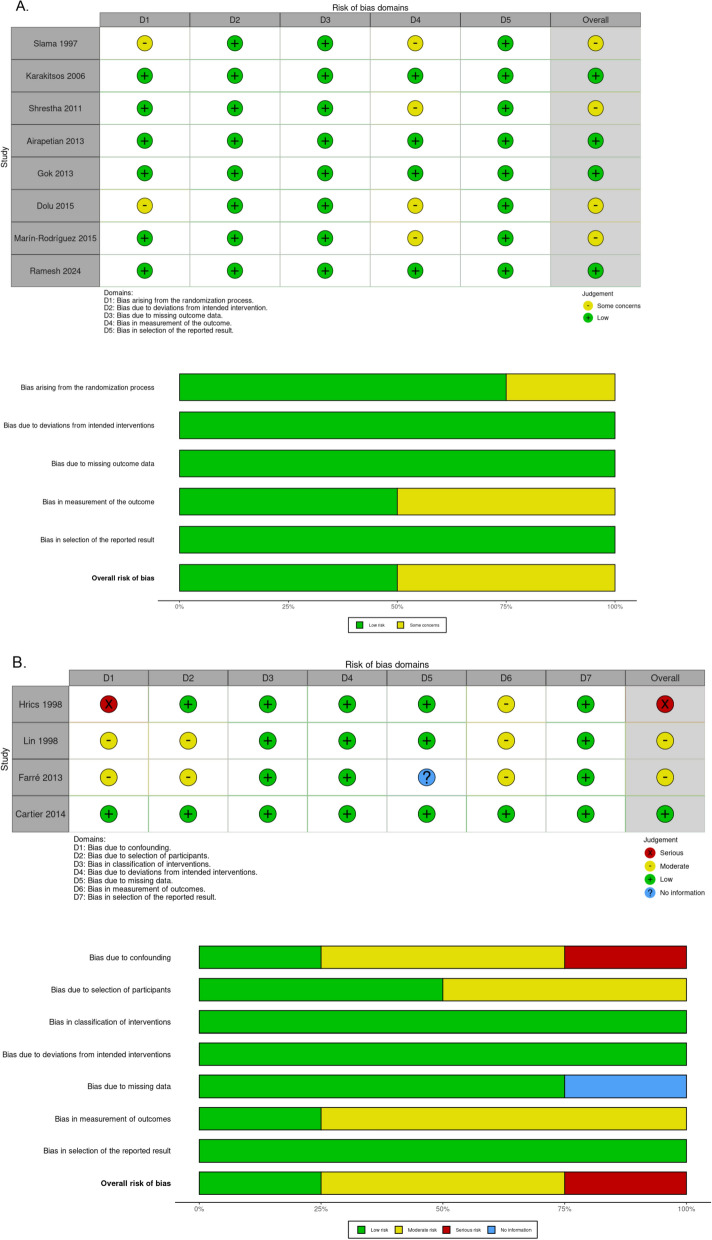
Methods: A systematic search on MEDLINE, Cochrane Central Register of Controlled Trials (CENTRAL), and Web of Science databases was conducted until July 31, 2024. Randomized controlled trials (RCTs) and non-randomized studies of intervention (NRSI) comparing US-guided versus AL-guided CVC placement were included. The primary outcome was a composite outcome including all types of catheter-related infection: catheter-related bloodstream infections (CRBSIs), central line-associated bloodstream infections (CLABSIs), catheter colonization, or any other type of reported infection. The secondary outcomes included individual infection types and mortality at day-28. Subgroup analyses based on study type and operator experience were also performed.
Results: Pooling twelve studies (8 RCTs and 4 NRSI), with a total of 5,092 CVC procedures (2072 US-guided and 3020 AL-guided), US-guided CVC was associated with a significant reduction in catheter-related infections compared with the AL technique (risk ratio (RR) = 0.68, 95% confidence interval (CI) 0.53-0.88). In the RCT subgroup, the pooled RR was 0.65 (95% CI 0.49-0.87). This effect was more pronounced in procedures performed by experienced operators (RR = 0.60, 95% CI 0.41-0.89). In inexperienced operators, the infection risk reduction was not statistically significant. The pooled analysis of CRBSIs and CLABSIs also favored US guidance (RR = 0.65, 95% CI 0.48-0.87).
Conclusion: US-guided CVC placement significantly reduces the risk of catheter-related infections compared to the AL technique, particularly when performed by experienced operators. Trial registration PROSPERO CRD42022350884. Registered 13 August 2022.
Keywords: Catheter-related bloodstream infection; Central venous catheterization; Meta-analysis; Ultrasound guidance.
© 2024. The Author(s).
Conflict of interest statement
Figures



References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
