

A multicentre prospective registry of one thousand sepsis patients admitted in Indian ICUs: (SEPSIS INDIA) study
- PMID: 39563464
- PMCID: PMC11577944
- DOI: 10.1186/s13054-024-05176-8
A multicentre prospective registry of one thousand sepsis patients admitted in Indian ICUs: (SEPSIS INDIA) study
Abstract
Background: Sepsis is a global health problem with high morbidity and mortality. Low- and middle-income countries have a higher incidence and poorer outcome with sepsis. Large epidemiological studies in sepsis using Sepsis-3 criteria, addressing the process of care and deriving predictors of mortality are scarce in India.
Method: A multicentre, prospective sepsis registry was conducted using Sepsis 3 criteria of suspected or confirmed infection and SOFA score of 2 or more in 19 ICUs in India over a period of one year (August 2022-July 2023). All adult patients admitted to the Intensive Care Unit who fulfilled the Sepsis 3 criteria for sepsis and septic shock were included. Patient infected with Covid 19 were excluded. Patients demographics, severity, admission details, initial resuscitation, laboratory and microbiological data and clinical outcome were recorded. Performance improvement programs as recommended by the Surviving Sepsis guideline were noted from the participating centers. Patients were followed till discharge or death while in hospital.
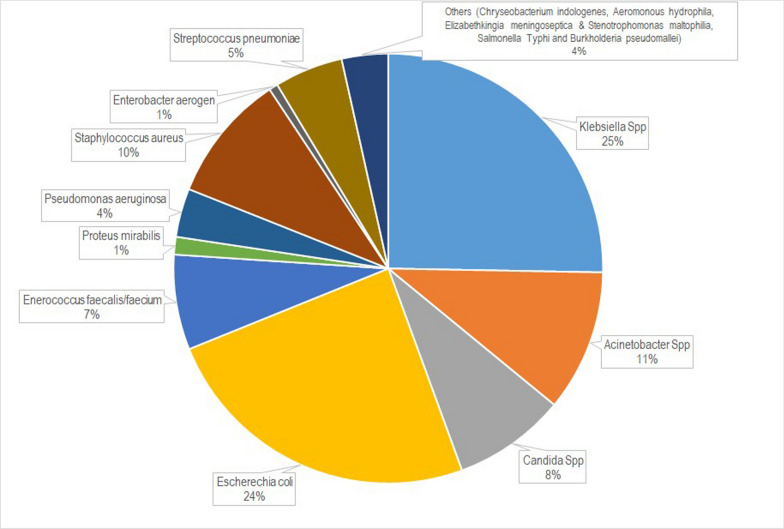
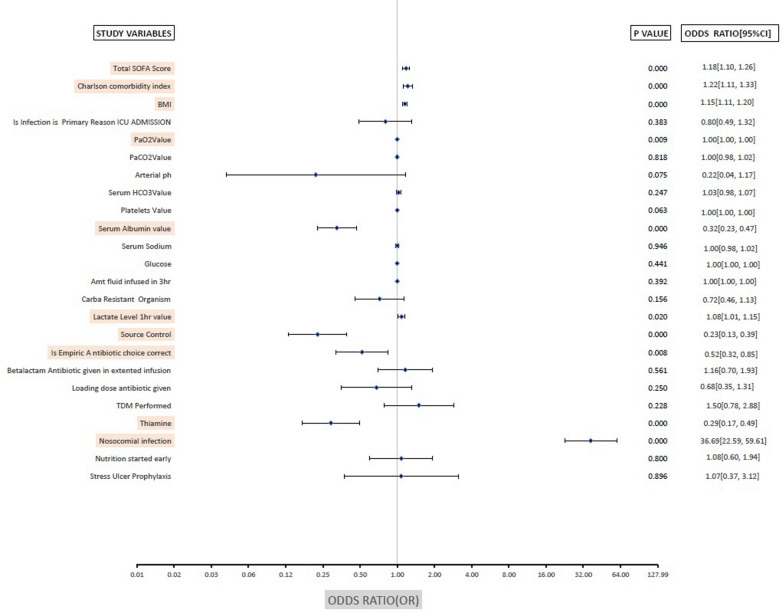
Results: Registry Data of 1172 patients with sepsis (including 500 patients with septic shock) were analysed. The average age of the study cohort was 65 years, and 61% were male. The average APACHE II and SOFA score was 21 and 6.7 respectively. The majority of patients had community-acquired infections, and lung infections were the most common source. Of all culture positive results, 65% were gram negative organism. Carbapenem-resistance was identified in 50% of the gram negative blood culture isolates. The predominant gram negative organisms were Klebsiella spp (25%), Escherechia coli (24%) and Acinetobacter Spp (11%). Tropical infections (Dengue, Malaria, Typhus) constituted minority (n = 32, 2.2%) of sepsis patients. The observed hospital mortality for the entire cohort (n = 1172) was 36.3%, for those without shock (n = 672) it was 25.6% and for those with shock (n = 500) it was 50.8%. The average length of ICU and hospital stay for the study cohort was 8.64 and 11.9 respectively. In multivariate analysis adequate source control, correct choice of empiric antibiotic and the use of intravenous thiamine were protective.
Conclusion: The general demographics of the sepsis population in the Indian Sepsis Registry is comparable to Western population. The mortality of sepsis cohort was higher (36.3%) but septic shock mortality (50.8%) was comparable to Western reports. Gram negative infection was the predominant cause of sepsis with a high incidence of carbapenem resistance. Eschericia coli, Klebsiella Spp and Acinetobacter Spp were the predominant causative organism. Tropical infection constituted a minority of sepsis population with low hospital mortality. The SOFA score on admission was a comparatively better predictor of poor outcome. Sepsis secondary to nosocomial infections had the worst outcomes, while source control, correct empirical antibiotic selection, and intravenous thiamine were protective. CTRI Registration CTRI:2022/07/044516.
Keywords: Epidemiology; India; Intensive Care Unit; Registry; Sepsis.
© 2024. The Author(s).
Conflict of interest statement
Figures
References
-
- Marshall JC, Vincent JL, Guyatt G, Angus DC, Abraham E, Bernard G, et al. Outcome measures for clinical research in sepsis: a report of the 2nd Cambridge colloquium of the international sepsis forum. Crit Care Med. 2005;33:1708–16. - PubMed
-
- Stephen AH, Montoya RL, Aluisio AR. Sepsis and septic shock in low- and middle-income countries. Surg Infect (Larchmt). 2020;21(7):571–8. - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
