

The outcome of surgery for congenital heart disease in India: A systematic review and metanalysis
- PMID: 39564152
- PMCID: PMC11573196
- DOI: 10.4103/apc.apc_71_24
The outcome of surgery for congenital heart disease in India: A systematic review and metanalysis
Abstract
Background: The mortality risks of children undergoing various cardiac surgeries for congenital heart disease (CHD) in India are not well defined. We conducted a systematic review and meta-analysis to estimate the inhospital mortality of various common CHD surgeries reported in India and compared it to representative data from established Western databases.
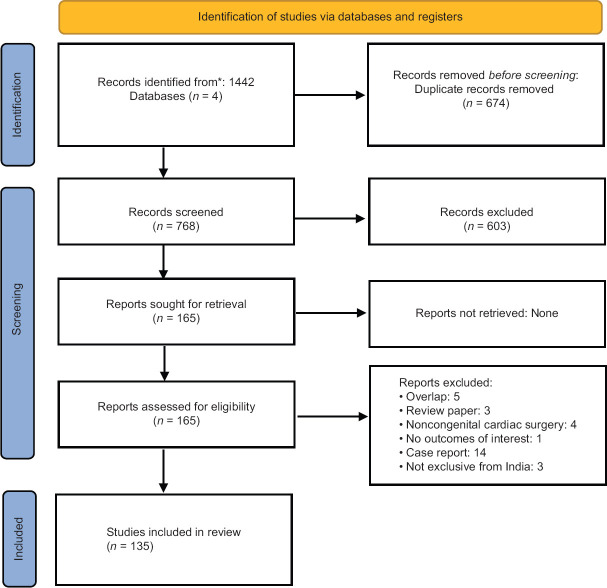
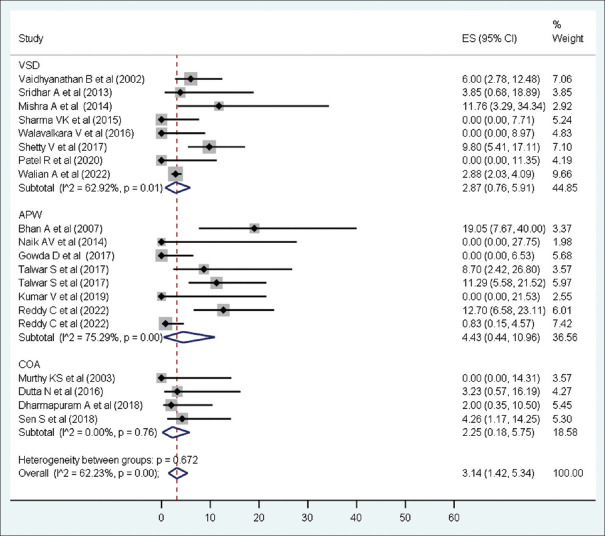
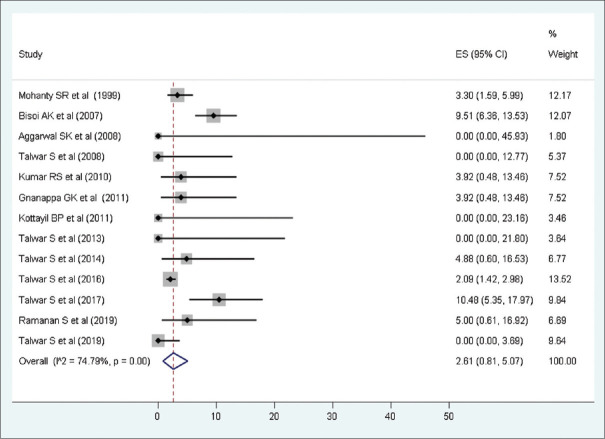
Methods and results: We searched four bibliographic databases for studies published in India over the last 25 years. In total, 135 studies met the inclusion criteria and included 30,587 patients aged from 1 day to 65 years. The pooled mortality rate of 43 Indian studies reporting multiple CHD surgical outcomes is 5.63% (95% confidence interval [CI]: 4.26-7.16; I 2 = 93.9%), whereas the Western data showed a pooled mortality rate of 2.65% (P value for comparison <0.0001). The pooled mortality risk for ventricular septal defect closure and tetralogy of Fallot repair in Indian studies was 2.87% (95% CI: 0.76-5.91; I 2 = 62.4%) and 4.61% (95% CI: 2.0-8.02; I 2 = 87.4%), respectively. The estimated mortality risk was higher than the Western databases for all subcategories studied except for surgeries in the grown-ups with CHD population and coarctation repair.
Conclusions: The estimated mortality risks are higher among Indian patients undergoing cardiac surgery for CHD as compared to Western data. We need prospective multicentric data to document whether the observed excess mortality exists after adjusting for various high-risk features and comorbidities in Indian patients. We need systemic measures to improve the outcomes of CHD surgeries in India.
Keywords: Operative mortality; congenital heart surgery; low- and middle-income countries; pooled mortality risk.
Copyright: © 2024 Annals of Pediatric Cardiology.
Conflict of interest statement
There are no conflicts of interest.
Figures



Comment in
-
Outcome of surgery for congenital heart disease - A perspective from Malaysia.Ann Pediatr Cardiol. 2024 Jul-Aug;17(4):229-230. doi: 10.4103/apc.apc_206_24. Epub 2024 Nov 15. Ann Pediatr Cardiol. 2024. PMID: 39698426 Free PMC article. No abstract available.
References
-
- Lawn JE, Cousens S, Zupan J Lancet Neonatal Survival Steering Team. 4 million neonatal deaths: When? Where? Why? Lancet. 2005;365:891–900. - PubMed
-
- Vaidyanathan B, Sathish G, Mohanan ST, Sundaram KR, Warrier KK, Kumar RK. Clinical screening for congenital heart disease at birth: A prospective study in a community hospital in Kerala. Indian Pediatr. 2011;48:25–30. - PubMed
-
- Saxena A. Congenital heart disease in India: A status report. Indian Pediatr. 2018;55:1075–82. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous