

Acute pancreatitis following asparaginase treatment in pediatric acute lymphoblastic leukemia with a heterozygous SPINK1 c.194 + 2T>C intronic variant: a case report
- PMID: 39564382
- PMCID: PMC11573588
- DOI: 10.3389/fped.2024.1493362
Acute pancreatitis following asparaginase treatment in pediatric acute lymphoblastic leukemia with a heterozygous SPINK1 c.194 + 2T>C intronic variant: a case report
Abstract
Background: Asparaginase is a critical component of chemotherapy for pediatric acute lymphoblastic leukemia (ALL), but its use is often complicated by asparaginase-associated pancreatitis (AAP). Genetic predispositions, such as variants in the SPINK1 gene, have been linked to an increased risk of pancreatitis. However, the role of genetic factors in relation to asparaginase treatment remains incompletely understood, partly because mutations in pancreatitis-causing genes are rarely found in pediatric ALL.
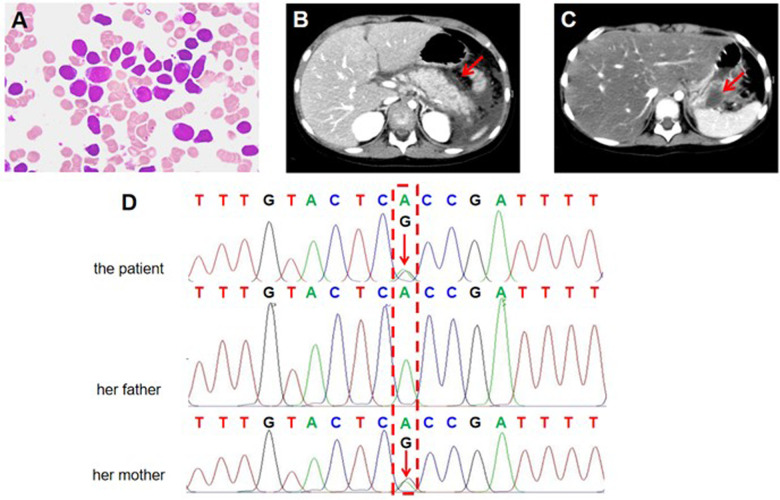
Case description: A four-year and three-month-old Chinese girl was admitted to our hospital due to fever for half a day, with no history of significant prior medical history. Initial blood tests revealed hematological abnormalities, including leukopenia, anemia, and thrombocytosis. Bone marrow aspiration identified 81.5% blast cells with B-lymphocyte morphology and immunophenotype, leading to a diagnosis of B-cell acute lymphoblastic leukemia (B-ALL). The patient began treatment under the CCCG-ALL-2015 protocol, which included PEG-asparaginase (PEG-asp). On day 10 of induction, she developed AAP, which was primarily characterized by severe epigastric pain and elevated serum amylase. Despite effective symptom management with analgesics and anti-inflammatory therapy, AAP recurred following administration of L-asparaginase (L-asp). Genetic analysis revealed a heterozygous SPINK1 c.194 + 2T>C variant (rs148954387), a well-known pathogenic variant associated with increased susceptibility to pancreatitis. Sanger sequencing confirmed that the SPINK1 variant was inherited from her asymptomatic mother. The patient's AAP was managed conservatively, and an asparaginase-free regimen ultimately achieved complete remission without recurrence of pancreatitis.
Conclusions: The identification of the SPINK1 c.194 + 2T>C variant, which is recognized as pathogenic, provides valuable information for understanding the heightened risk of AAP in our pediatric ALL patient. Our case underscores the potential role of genetic predisposition in the development of AAP and highlights the importance of considering genetic screening prior to asparaginase therapy in pediatric ALL patients to identify those at increased risk.
Keywords: SPINK1; acute lymphoblastic leukemia; asparaginase; c.194 + 2T>C; case report; pancreatitis.
© 2024 Zhou, Lu, Wang, Gu, Li and Zhao.
Conflict of interest statement
TW was employed by Dian Diagnostics Group Co., Ltd. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Peg-Asparaginase-Associated Pancreatitis in Chemotherapy-Treated Pediatric Patients: A 5-Year Retrospective Study.Front Oncol. 2020 Oct 28;10:538779. doi: 10.3389/fonc.2020.538779. eCollection 2020. Front Oncol. 2020. Retraction in: Front Oncol. 2021 Jun 03;11:709636. doi: 10.3389/fonc.2021.709636. PMID: 33194600 Free PMC article. Retracted.
-
Acute pancreatitis in children with acute lymphoblastic leukemia correlates with L-asparaginase dose intensity.Pediatr Res. 2022 Aug;92(2):459-465. doi: 10.1038/s41390-021-01796-w. Epub 2021 Oct 30. Pediatr Res. 2022. PMID: 34718353
-
Clinical summary of pediatric acute lymphoblastic leukemia patients complicated with asparaginase-associated pancreatitis in SCCLG-ALL-2016 protocol.Hematology. 2023 Dec;28(1):2171723. doi: 10.1080/16078454.2023.2171723. Hematology. 2023. PMID: 36752506
-
Asparaginase-Associated Pancreatitis in Pediatric Patients with Acute Lymphoblastic Leukemia: Current Perspectives.Paediatr Drugs. 2021 Sep;23(5):457-463. doi: 10.1007/s40272-021-00463-1. Epub 2021 Aug 5. Paediatr Drugs. 2021. PMID: 34351604 Review.
-
[A case of ALL complicated with acute pancreatitis and pancreatic pseudocyst caused by L-asparaginase ].Gan To Kagaku Ryoho. 1993 Jan;20(1):149-52. Gan To Kagaku Ryoho. 1993. PMID: 8422180 Review. Japanese.
References
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous