

Enterovirus A71 and coxsackievirus A6 circulation in England, UK, 2006-2017: A mathematical modelling study using cross-sectional seroprevalence data
- PMID: 39565769
- PMCID: PMC11578500
- DOI: 10.1371/journal.ppat.1012703
Enterovirus A71 and coxsackievirus A6 circulation in England, UK, 2006-2017: A mathematical modelling study using cross-sectional seroprevalence data
Abstract
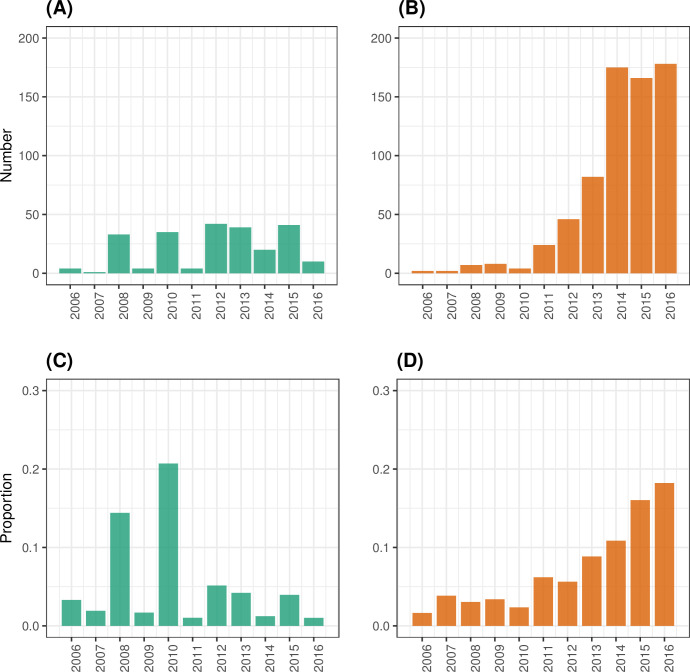
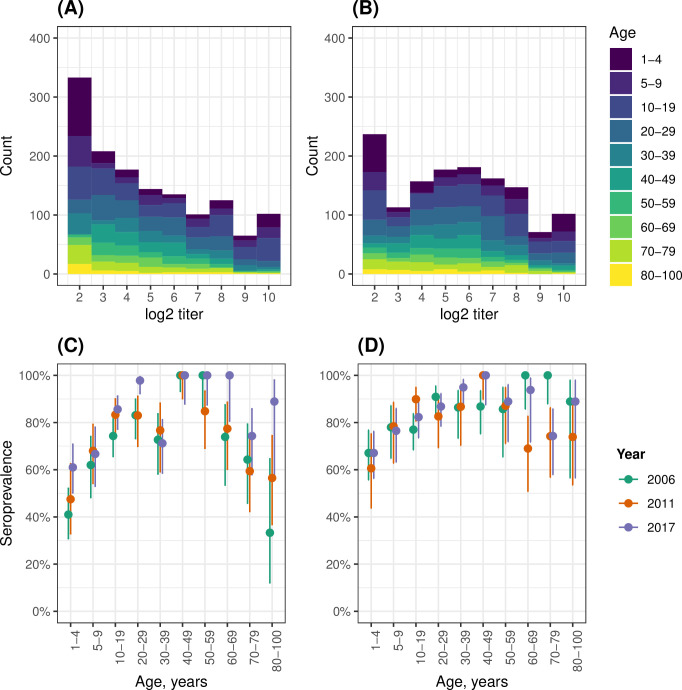
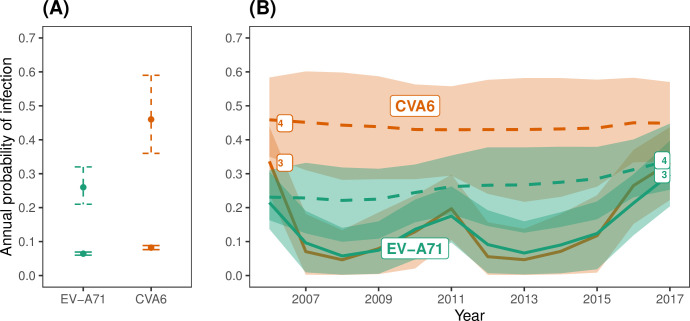
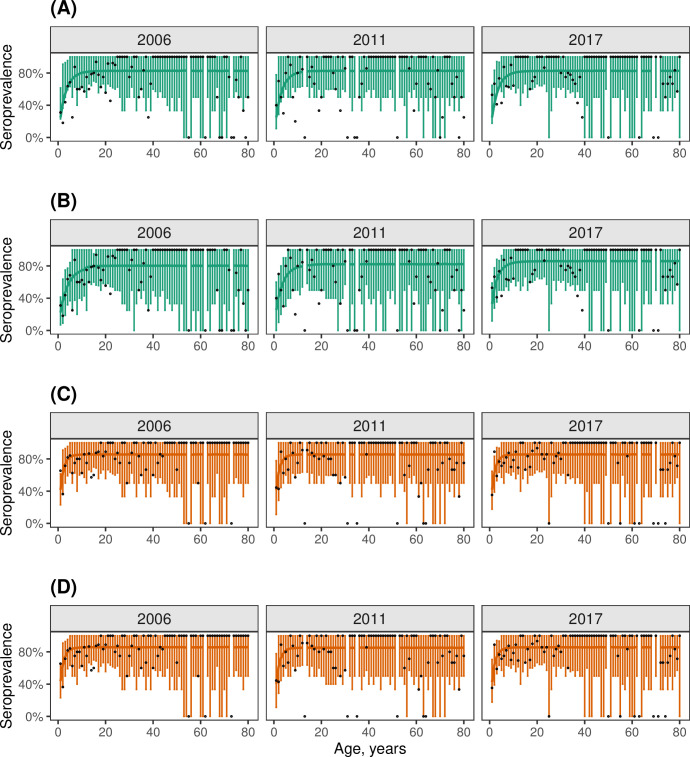
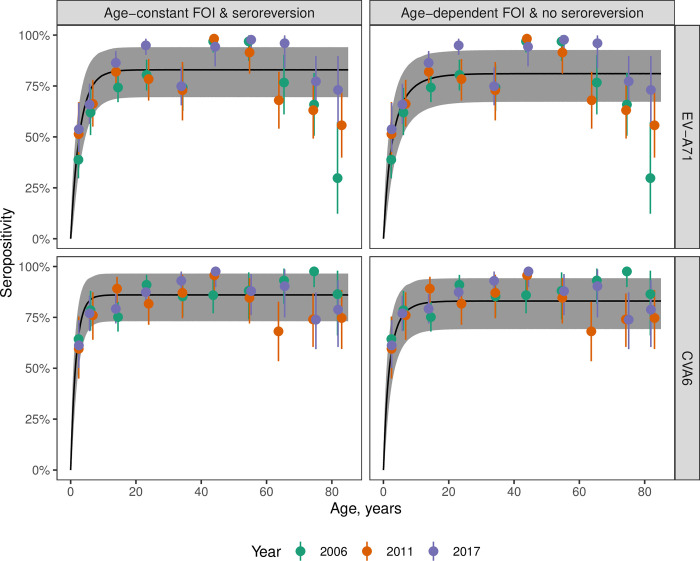
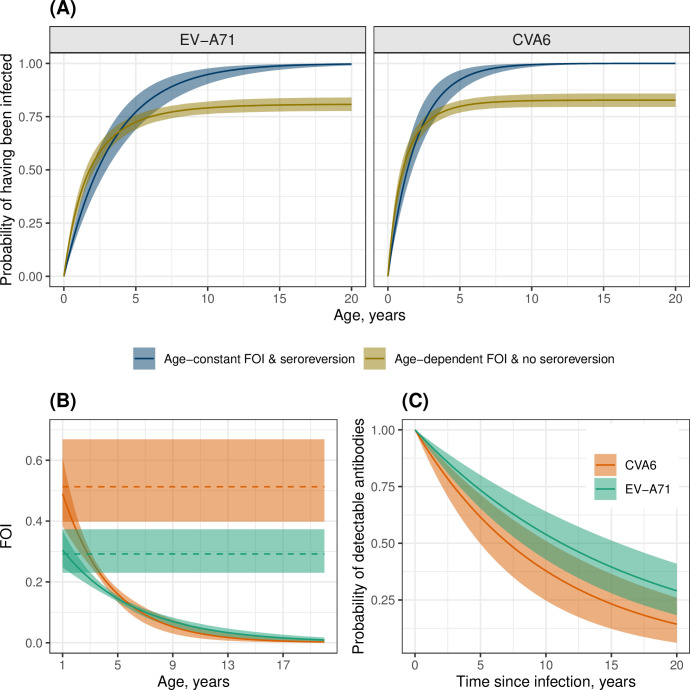
Enterovirus A71 (EV-A71) and coxsackievirus A6 (CVA6) primarily cause hand, foot and mouth disease and have emerged to cause potential fatal neurological and systemic manifestations. However, limited surveillance data collected through passive surveillance systems hampers characterization of their epidemiological dynamics. We fit a series of catalytic models to age-stratified seroprevalence data for EV-A71 and CVA6 collected in England at three time points (2006, 2011 and 2017) to estimate the force of infection (FOI) over time and assess possible changes in transmission. For both serotypes, model comparison does not support the occurrence of important changes in transmission over the study period, and we find that a declining risk of infection with age and / or seroreversion are needed to explain the seroprevalence data. Furthermore, we provide evidence that the increased number of reports of CVA6 during 2006-2017 is unlikely to be explained by changes in surveillance. Therefore, we hypothesize that the increased number of CVA6 cases observed since 2011 must be explained by increased virus pathogenicity. Further studies of seroprevalence data from other countries would allow to confirm this. Our results underscore the value of seroprevalence data to unravel changes in the circulation dynamics of pathogens with weak surveillance systems and large number of asymptomatic infections.
Copyright: © 2024 Kamau et al. This is an open access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
