

Association between admission baseline blood potassium levels and all-cause mortality in patients with acute kidney injury combined with sepsis: A retrospective cohort study
- PMID: 39565797
- PMCID: PMC11578480
- DOI: 10.1371/journal.pone.0309764
Association between admission baseline blood potassium levels and all-cause mortality in patients with acute kidney injury combined with sepsis: A retrospective cohort study
Abstract
Introduction: Imbalances in blood potassium (K) homeostasis is a significant contributor to the emergence of severe complications, especially among critically ill patients. Hypokalemia and hyperkalemia are both associated with an increased risk of adverse events. However, it is not known about the impact of blood K levels on risk of intensive care units (ICU) mortality for Acute kidney injury (AKI) combined with sepsis patients. This study aimed to explore the relationship between admission blood K levels and ICU 30-day mortality in patients with AKI combined with sepsis.
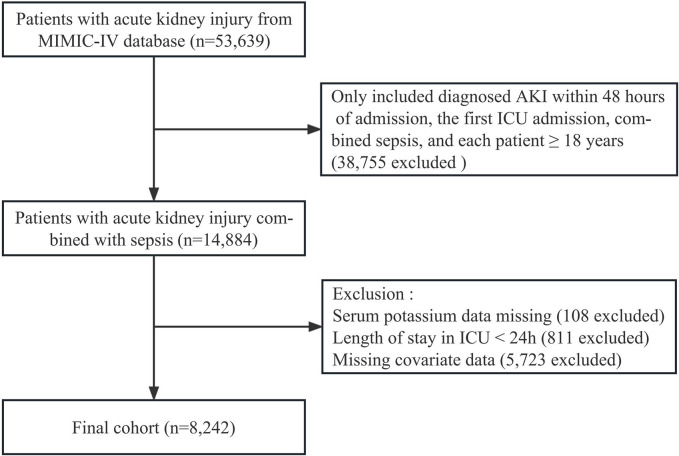
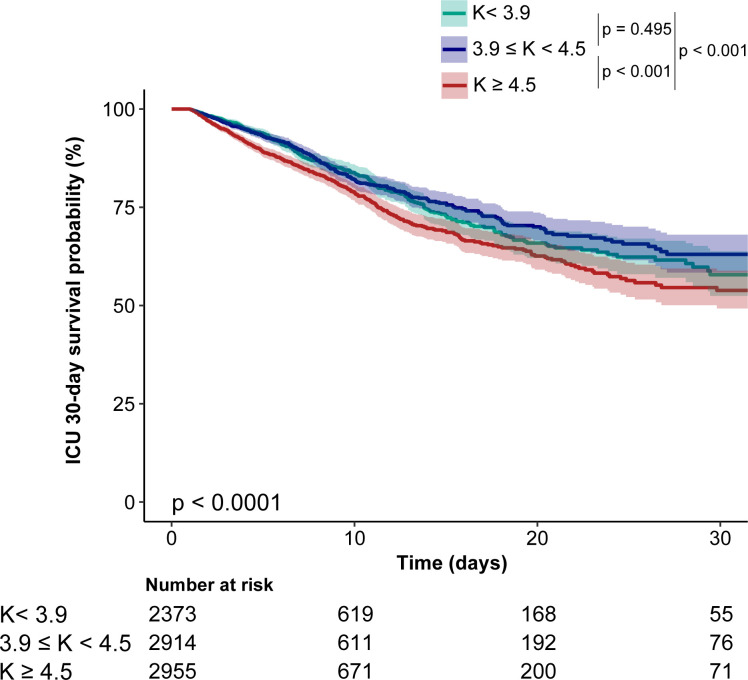
Methods: We selected patients diagnosed with AKI and sepsis on their first ICU admission from the Medical Information Mart for Intensive Care IV (MIMIC-IV) database. The first blood K levels within 24 hours of admission were categorized into three groups according to tertiles (T1 < 3.9 mmol/L, 3.9 ≤ T2 < 4.5 mmol/L, and T3 ≥ 4.5 mmol/L), with T2 serving as the reference. We examined the association between blood K levels and ICU 30-day mortality using accelerated failure time (AFT) models and survival analysis.
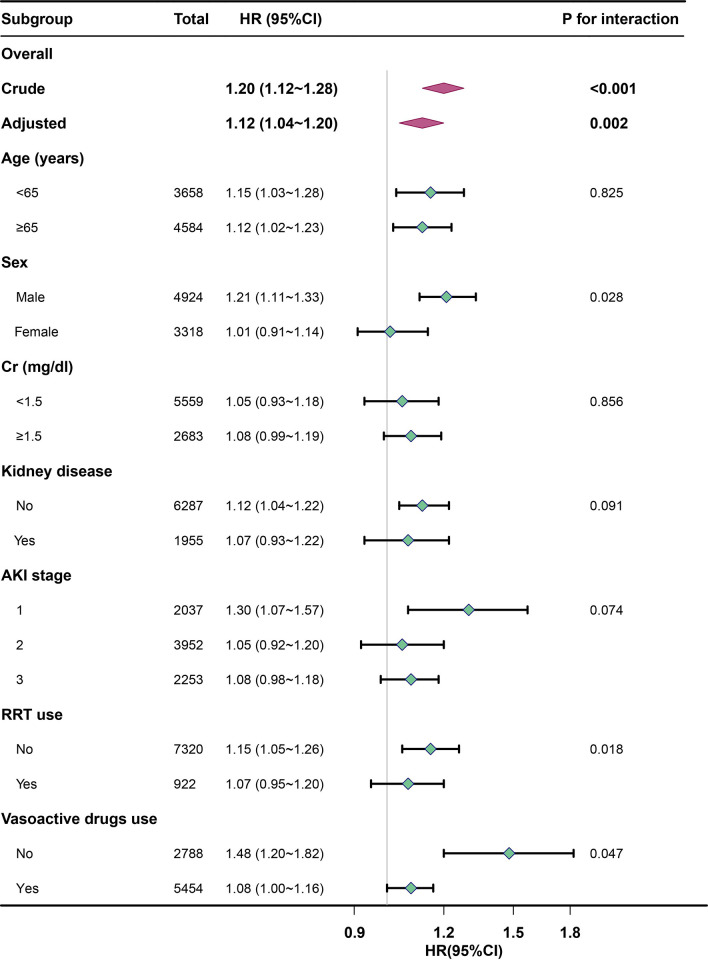
Results: A total of 8,242 ICU patients with AKI combined with sepsis were included. In multivariate AFT models, each 1 mmol/L increase in blood K levels was associated with a 13% increase in the risk of ICU 30-day mortality (p < 0.001, 95% confidence interval (CI): 1.06-1.20). Extended multivariable AFT models showed that, compared to the middle category, patients with high blood K levels (≥ 4.5 mmol/L) were associated with all-cause mortality (p = 0.002, adjusted hazard ratio (HR) = 1.22, 95% CI: 1.08-1.38), whereas those with low blood K levels (< 3.9 mmol/L) showed no significant difference (p = 0.385, adjusted HR = 1.06, 95% CI: 0.93-1.21). Kaplan-Meier curves indicated that patients with high blood K levels had higher mortality, and those with middle blood potassium levels (3.9 ≤ K < 4.5 mmol/L) had the lowest mortality.
Conclusion: The admission baseline blood K levels were significantly associated with ICU 30-day mortality in intensive care patients suffering from AKI in conjunction with sepsis. Therefore, immediate and careful correction of blood potassium imbalances may prove to be a crucial approach in improving outcomes for these patients.
Copyright: © 2024 Guo et al. This is an open access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
Similar articles
-
Albumin corrected anion gap and clinical outcomes in elderly patients with acute kidney injury caused or accompanied by sepsis: a MIMIC-IV retrospective study.Eur J Med Res. 2025 Jan 7;30(1):11. doi: 10.1186/s40001-024-02238-z. Eur J Med Res. 2025. PMID: 39773636 Free PMC article.
-
Admission serum sodium and potassium levels predict survival among critically ill patients with acute kidney injury: a cohort study.BMC Nephrol. 2019 Aug 8;20(1):311. doi: 10.1186/s12882-019-1505-9. BMC Nephrol. 2019. PMID: 31395027 Free PMC article.
-
[A multicenter clinical study of critically ill patients with sepsis complicated with acute kidney injury in Beijing: incidence, clinical characteristics and outcomes].Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2024 Jun;36(6):567-573. doi: 10.3760/cma.j.cn121430-20240210-00124. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2024. PMID: 38991953 Chinese.
-
Influence of dyskalemia at admission and early dyskalemia correction on survival and cardiac events of critically ill patients.Crit Care. 2019 Dec 19;23(1):415. doi: 10.1186/s13054-019-2679-z. Crit Care. 2019. PMID: 31856891 Free PMC article.
-
Association between the mean perfusion pressure and the risk of acute kidney injury in critically ill patients with sepsis: a retrospective cohort study.BMC Infect Dis. 2024 Aug 9;24(1):806. doi: 10.1186/s12879-024-09706-1. BMC Infect Dis. 2024. PMID: 39123120 Free PMC article.
Cited by
-
Predictive Nomogram for Acute Kidney Injury Risk with Vancomycin and Piperacillin Tazobactam in Sepsis Treatment.Med Sci Monit. 2025 Jul 4;31:e949340. doi: 10.12659/MSM.949340. Med Sci Monit. 2025. PMID: 40611514 Free PMC article.
-
Association between serum glucose potassium ratio and short- and long-term all-cause mortality in patients with sepsis admitted to the intensive care unit: a retrospective analysis based on the MIMIC-IV database.Front Endocrinol (Lausanne). 2025 Jul 30;16:1555082. doi: 10.3389/fendo.2025.1555082. eCollection 2025. Front Endocrinol (Lausanne). 2025. PMID: 40810063 Free PMC article.
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
