

doi: 10.1056/NEJMc2409428.
Diagnostic Complexity in Monoclonal Gammopathy of Thrombotic Significance
Affiliations
- PMID: 39565997
- PMCID: PMC11581683
- DOI: 10.1056/NEJMc2409428
Item in Clipboard
Diagnostic Complexity in Monoclonal Gammopathy of Thrombotic Significance
N Engl J Med.
.
No abstract available
Figures
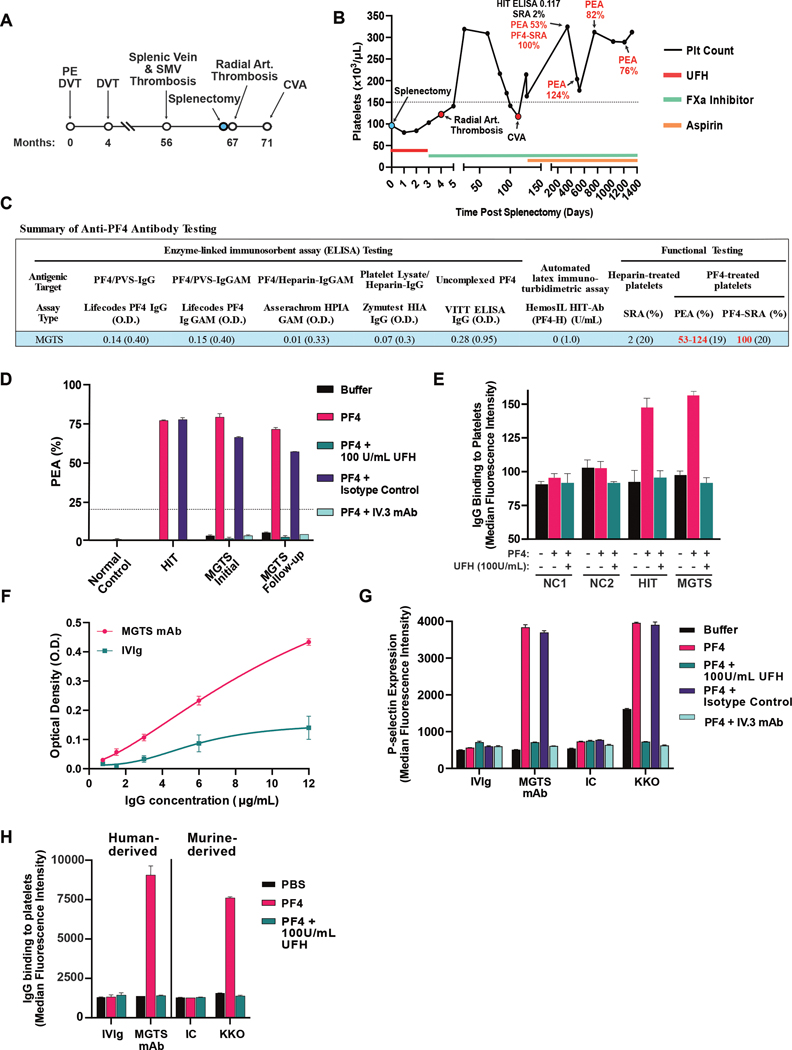
(A) Elapsed time from the onset of thrombotic episodes and details of thromboses are displayed. The patient underwent splenectomy for hypersplenism secondary to splenic vein thrombosis (blue circle). (B) Available platelet counts around periods of thrombosis are displayed. Red circles denote major clinical events. Patient treatment with anticoagulation/antiplatelet medications is listed at the bottom of the graph. Positive test results are denoted in red font. (C) Results from several HIT antigen-based immunoassays, a VITT-specific ELISA employing uncomplexed PF43, and functional testing results (PEA, SRA, and PF4-SRA) are shown. Positive test results are denoted in red font, negative results in black font, and positive assay cut-offs are enclosed in parentheses. (D) PEA testing results are displayed for two patient samples obtained several months apart in the following testing conditions: Buffer-treated platelets, PF4-treated platelets, PF4-treated platelets with high concentration of unfractionated heparin (UFH, 100 U/mL), PF4-treated platelets with an isotype control (IC) murine monoclonal antibody, or PF4-treated platelets with the FcGRIIa-blocking murine monoclonal antibody IV.3. PF4-dependent activation was inhibited by both high concentrations of heparin and FcGRIIa blockade. HIT-HIT positive control. (E) Quantification of IgG binding to platelets is displayed for two healthy donor samples (NC1, NC2), serum from a patient confirmed to have heparin-induced thrombocytopenia (HIT), and serum from the MGTS patient for the following testing conditions: Buffer-treated platelets, PF4-treated platelets, PF4-treated platelets with high concentration of unfractionated heparin (UFH, 100 U/mL). (F) The binding of recombinant patient antibody (MGTS mAb) or pooled human immunoglobulin G (intravenous immunoglobulin, IVIg) to PF4/polyanion complexes was assessed at several concentrations in the Lifecodes PF4 IgG HIT ELISA. (G) PEA results are displayed for the recombinant patient antibody (MGTS mAb), IVIg, an isotype control murine monoclonal antibody (IC), and for a HIT-like murine monoclonal antibody (KKO) in the following conditions: Buffer-treated platelets, PF4-treated platelets, PF4-treated platelets with high concentration of unfractionated heparin (UFH, 100 U/mL), PF4-treated platelets with an isotype control (IC) murine monoclonal antibody, or PF4-treated platelets with the FcGRIIa-blocking murine monoclonal antibody IV.3. PF4-dependent activation was inhibited by both high concentration of heparin and FcGRIIa blockade. KKO, a murine monoclonal HIT-like antibody activates platelets as expected while Intravenous immunoglobulin G (IVIg) does not. (H) Quantification of IgG binding to platelets is displayed for recombinant patient antibody (MGTS mAb), IVIg, an isotype control murine monoclonal antibody (IC), and for a HIT-like murine monoclonal antibody (KKO) for the following testing conditions: Buffer-treated platelets, PF4-treated platelets, PF4-treated platelets with high concentration of unfractionated heparin (UFH, 100 U/mL). Additional note: Patient testing showed no evidence of a lupus anticoagulant or deficiency of Antithrombin, Protein C, or Protein S. The patient was also negative for anticardiolipin and anti-beta 2 glycoprotein I antibodies (IgG and IgM isotypes). There was no evidence of resistance to activated protein C (APC), therefore, DNA-based testing for the factor V Leiden variant was not performed. A normal APC resistance ratio has a greater than 99% negative predictive value for factor V Leiden variant. The patient was also negative for the Prothrombin G20210A variant.
References
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources