

Thrombopoietic agents enhance bone healing in mice, rats, and pigs
- PMID: 39566068
- PMCID: PMC11700610
- DOI: 10.1093/jbmr/zjae191
Thrombopoietic agents enhance bone healing in mice, rats, and pigs
Abstract
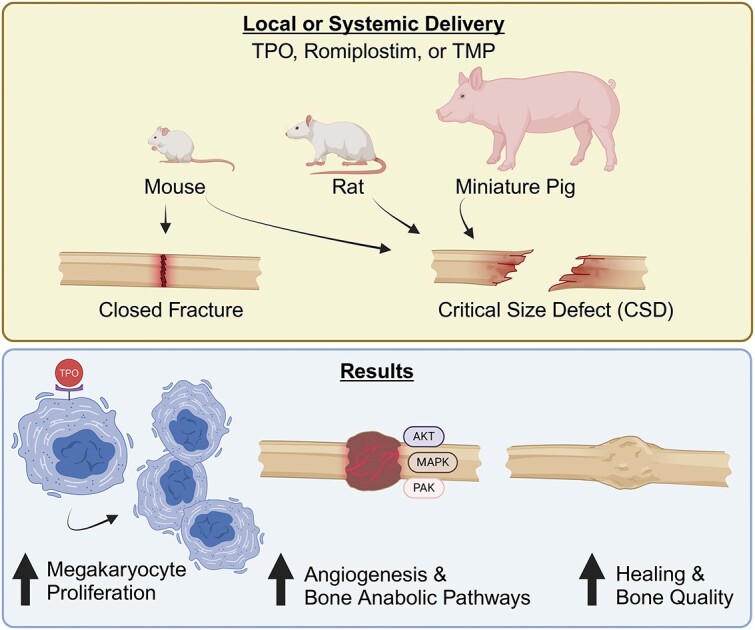
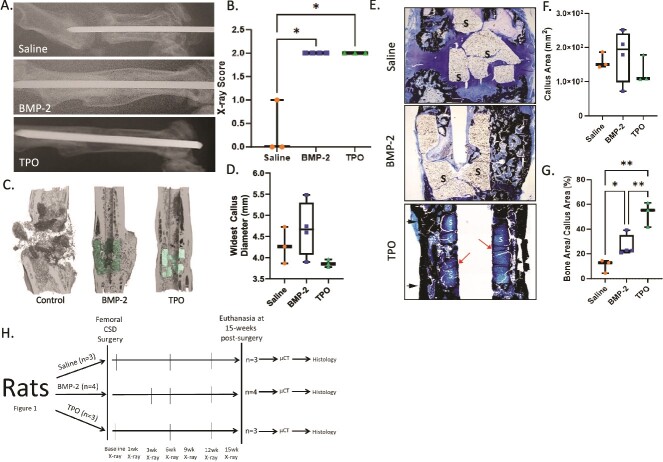
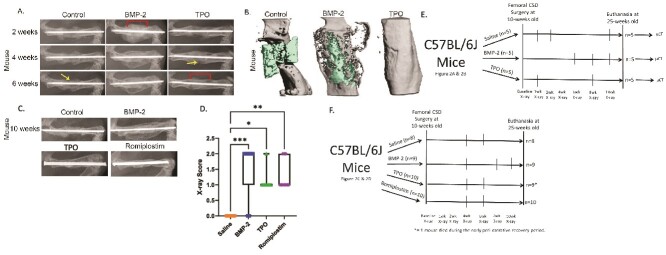
Achieving bone union remains a significant clinical dilemma. The use of osteoinductive agents, specifically bone morphogenetic proteins (BMPs), has gained wide attention. However, multiple side effects, including increased incidence of cancer, have renewed interest in investigating alternatives that provide safer, yet effective bone regeneration. Here we demonstrate the robust bone healing capabilities of the main megakaryocyte (MK) growth factor, thrombopoietin (TPO), and second-generation TPO agents using multiple animal models, including mice, rats, and pigs. This bone healing activity is shown in two fracture models (critical-sized defect [CSD] and closed fracture) and with local or systemic administration. Our transcriptomic analyses, cellular studies, and protein arrays demonstrate that TPO enhances multiple cellular processes important to fracture healing, particularly angiogenesis, which is required for bone union. Finally, the therapeutic potential of thrombopoietic agents is high since they are used in the clinic for other indications (eg, thrombocytopenia) with established safety profiles and act upon a narrowly defined population of cells.
Keywords: bone healing; bone regeneration; bone repair; fracture; thrombopoietin.
Plain language summary
Fractures that fail to heal can be devasting injuries. Treatment options are limited and center on stimulating bone growth. However, this treatment does not fully stimulate the many cell types in natural healing. Megakaryocytes (MKs) are “first responders” to injury and begin the healing process. We have investigated delivering thrombopoietic agents, which stimulate MK growth, directly to fractures incapable of healing. We found these agents can aid in healing such fractures in mice, rats, and pigs. Thrombopoietic agents are currently Food and Drug Administration (FDA)-approved for certain blood conditions. Our work suggests repurposing these agents to help heal fractures that may otherwise never heal.
© The Author(s) 2024. Published by Oxford University Press on behalf of the American Society for Bone and Mineral Research.
Conflict of interest statement
M.A.K. and T.-M.G.C. are co-inventors on a patent for the use of thrombopoietic agents in bone healing. M.A.K. is the founder of OsteoFuse, LLC. For all other authors, no conflicts of interest exist.
Figures




References
MeSH terms
Substances
Grants and funding
- R01 AG060621/AG/NIA NIH HHS/United States
- UL1 RR025761/RR/NCRR NIH HHS/United States
- AG060621/GF/NIH HHS/United States
- R01 AR060332/AR/NIAMS NIH HHS/United States
- UL1 TR000006/TR/NCATS NIH HHS/United States
- IK6 RX004809/RX/RRD VA/United States
- I01 BX006399/BX/BLRD VA/United States
- I01 BX003751/BX/BLRD VA/United States
- TR000006/Indiana Clinical and Translational Sciences Institute
- W81XWH-13-1-0501/Orthopaedic Trauma Association
- R01 AR060863/AR/NIAMS NIH HHS/United States
- T32 DK007519/DK/NIDDK NIH HHS/United States
LinkOut - more resources
Full Text Sources
