

The presentation and treatment of Dupuytren's disease in Dutch general practitioner care
- PMID: 39566072
- PMCID: PMC11811527
- DOI: 10.1093/fampra/cmae065
The presentation and treatment of Dupuytren's disease in Dutch general practitioner care
Abstract
Background: When research and management of Dupuytren's disease (DD) shift from symptom relief to preventing contractures, general practitioner (GP) care may become more central to treatment. However, the presentation and course of DD in GP care are underexplored and this has been recognized as a knowledge gap that hinders effective treatment decisions. This study is the first to map the trajectory of DD patients in GP care.
Methods: Using electronic health records from Dutch general practices in a regional research network, we conducted a registration-based cohort study in a dynamic population. Descriptive statistics detailed patient demographics, number of contacts, and symptoms per contact. The time and number of contacts before diagnosis were also analysed. Sankey diagrams illustrated the relationship between management options and symptoms.
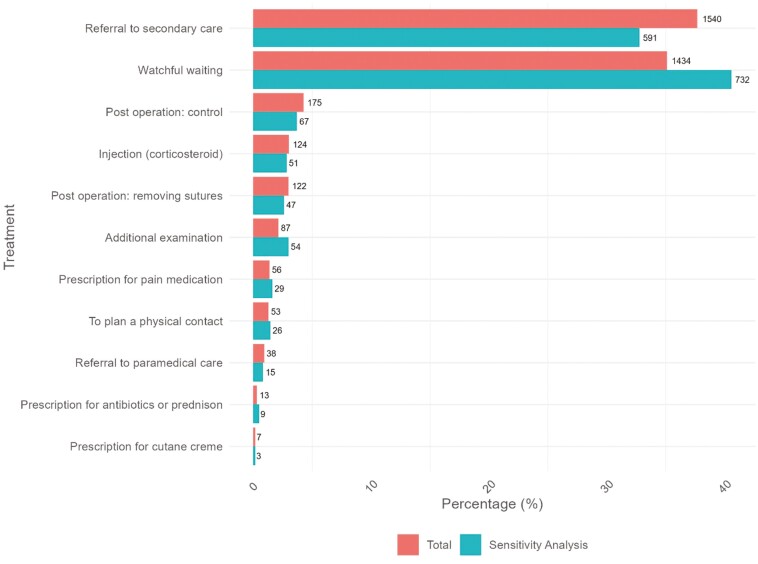
Results: Over a 16-year period, 84% of patients with a DD diagnosis had visited their GP for this reason, with 73% only having one GP contact. The diagnosis was made at first contact for 93% of patients. Initial contacts often reported a lump (57.3%), but this symptom was less frequent in subsequent visits. 'Daily life impairment' increased after the first contact. The most common management options were referral to secondary care (37.7%) and watchful waiting (35.1%).
Conclusion: The diagnosis and management of DD in GP care are in line with the current guidelines. Less than half of the DD patients were referred to secondary care during follow-up. This may give room for preventive treatment that limits progression. Future studies should focus on the accuracy of diagnosis and the feasibility of effective treatments in GP care.
Keywords: Dupuytren’s contracture; epidemiology; primary care; symptoms; treatment.
© The Author(s) 2024. Published by Oxford University Press.
Conflict of interest statement
PW is a member of the Data Monitoring Committee of Fidia Ltd, Milan, Italy. PW is a member of the scientific advisory board of the International Dupuytren Society, and PW and DB are or were both members of the scientific advisory board of the Dutch Dupuytren Society. These interests are not related to the submitted work. All other authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures


References
-
- Elliot D. The early history of Dupuytren’s disease. Hand Clin 1999;15:1–19, v. - PubMed
-
- Rayan GM. Dupuytren disease: anatomy, pathology, presentation and treatment. J Bone Joint Surg Am 2004;89:189–98. https://doi.org/ 10.2106/00004623-200701000-00026 - DOI - PubMed
-
- Broekstra DC, Lanting R, Werker PMN, et al. Disease course of primary Dupuytren disease: 5-year results of a prospective cohort study. Plast Reconstr Surg 2022;149:1371–8. https://doi.org/ 10.1097/PRS.0000000000009115 - DOI - PubMed
-
- Reilly RM, Stern PJ, Goldfarb CA.. A retrospective review of the management of Dupuytren’s nodules. J Hand Surg 2005;30:1014–8. https://doi.org/ 10.1016/j.jhsa.2005.03.005 - DOI - PubMed
-
- Gudmundsson KG, Arngrímsson R, Jónsson T.. Eighteen years follow-up study of the clinical manifestations and progression of Dupuytren’s disease. Scand J Rheumatol 2001;30:31–4. https://doi.org/ 10.1080/030097401750065292 - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
