

Positive Antiganglioside Antibodies in a Patient with Primary Diffuse Large B-cell Lymphoma of the Central Nervous System
- PMID: 39566992
- PMCID: PMC12241723
- DOI: 10.2169/internalmedicine.2326-23
Positive Antiganglioside Antibodies in a Patient with Primary Diffuse Large B-cell Lymphoma of the Central Nervous System
Abstract
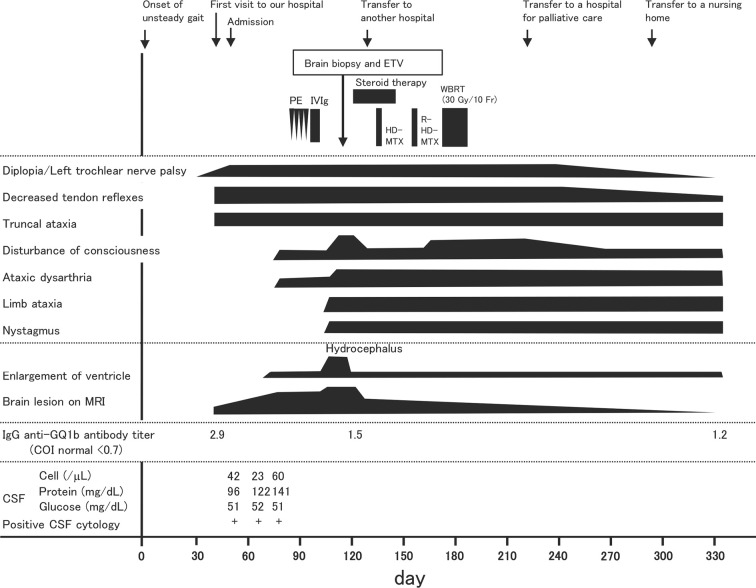
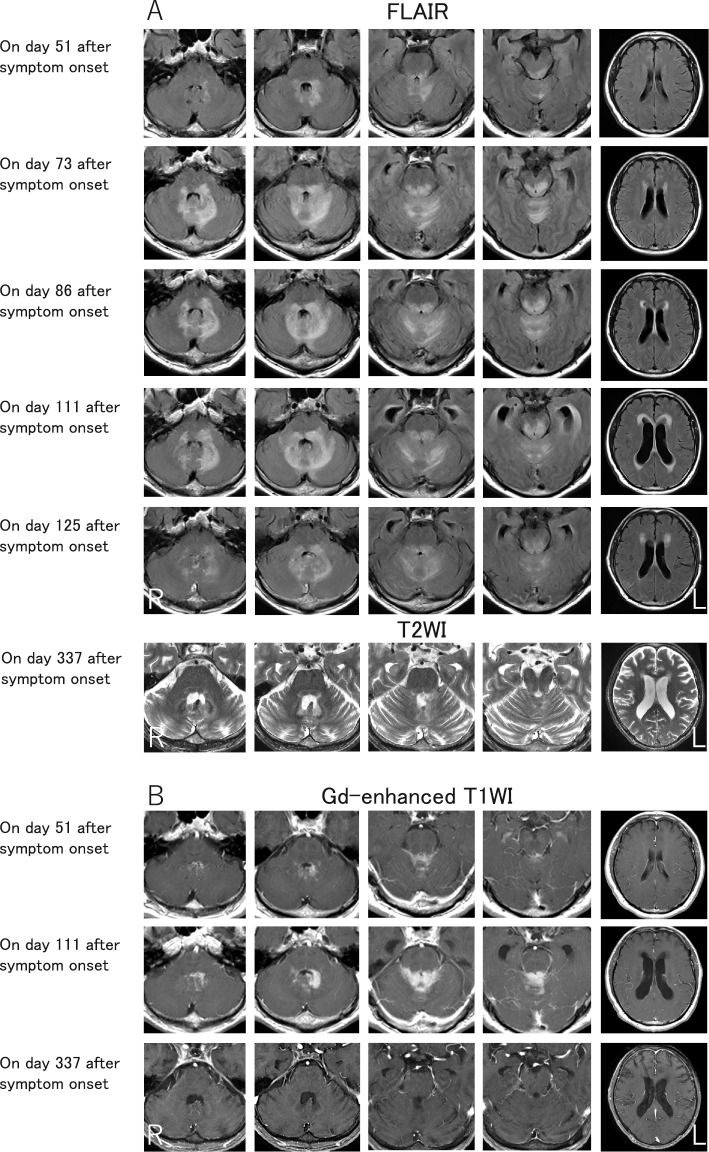
Up to one-third of lymphoma cases involve the nervous system. Miller-Fisher syndrome (MFS) associated with lymphoma is extremely rare. We herein report a case of primary central nervous system lymphoma initially mimicking MFS in a 70-year-old man who presented with subacute unsteady gait and diplopia. A neurological examination revealed unilateral ophthalmoplegia, ataxia, and areflexia. The patient tested positive for anti-GQ1b antibodies, so MFS was initially suspected. However, the progression extended over one month. Subsequently, disturbance of consciousness was observed. Cranial magnetic resonance imaging revealed lesions in the periventricular fourth ventricle, and a brain biopsy indicated diffuse large B-cell lymphoma.
Keywords: Bickerstaff brainstem encephalitis; Miller-Fisher syndrome; anti-GQ1b antibody; anti-GQ1b syndrome; diffuse large B-cell lymphoma; primary central nervous system lymphoma.
Conflict of interest statement
The authors state that they have no Conflict of Interest (COI).
Figures

References
-
- Mauermann ML. Neurologic complications of lymphoma, leukemia, and paraproteinemias. Continuum (Minneap Minn) 23(3, Neurology of Systemic Disease): 669-690, 2017. - PubMed
-
- Giglio P, Gilbert MR. Neurologic complications of non-Hodgkin's lymphoma. Curr Hematol Malig Rep 1: 214-219, 2006. - PubMed
-
- Makranz C, Arkadir D, Nachmias B, et al. Neurological misdiagnoses of lymphoma. Neurol Sci 42: 1933-1940, 2021. - PubMed
-
- Nayak L, Batchelor TT. How I treat neurologic complications in patients with lymphoid cancer. Blood 139: 1469-1478, 2022. - PubMed
-
- Tomita M, Koike H, Kawagashira Y, et al. Clinicopathological features of neuropathy associated with lymphoma. Brain 136: 2563-2578, 2013. - PubMed