

Future Health Today and patients at risk of undiagnosed cancer: a pragmatic cluster randomised trial of quality- improvement activities in general practice
- PMID: 39567181
- PMCID: PMC12010534
- DOI: 10.3399/BJGP.2024.0491
Future Health Today and patients at risk of undiagnosed cancer: a pragmatic cluster randomised trial of quality- improvement activities in general practice
Abstract
Background: Diagnosing cancer in general practice is complex, given the non-specific nature of many presenting symptoms and the overlap of potential diagnoses.
Aim: This trial aimed to evaluate the effectiveness of Future Health Today (FHT) - a technology that provides clinical decision support, auditing, and quality-improvement monitoring - on the appropriate follow-up of patients at risk of undiagnosed cancer.
Design and setting: Pragmatic, cluster randomised trial undertaken in general practices in Victoria and Tasmania, Australia.
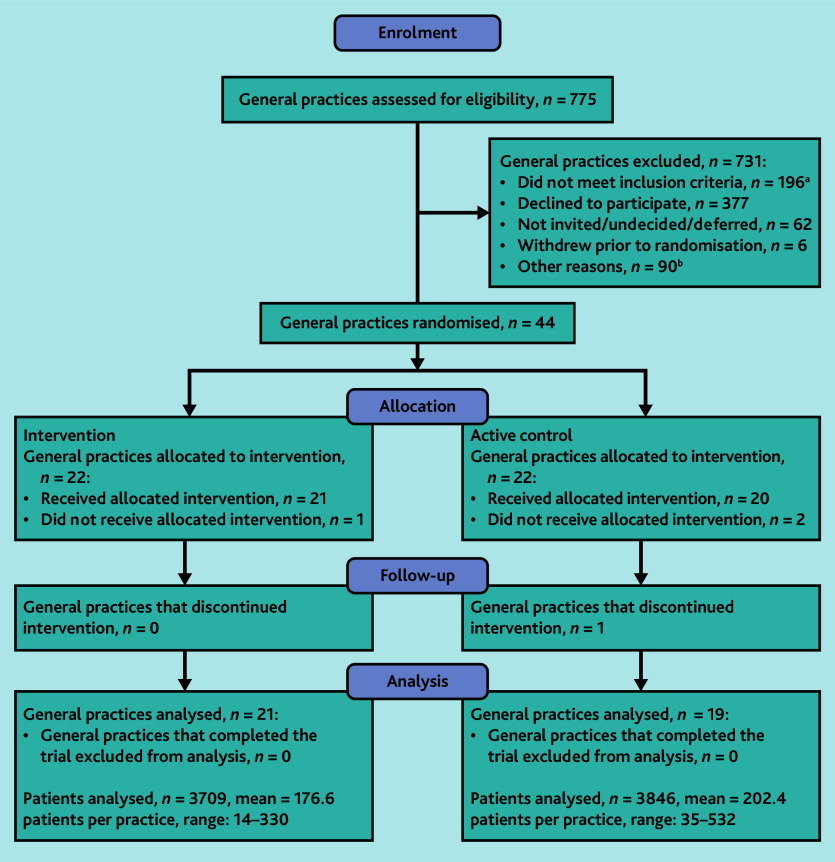
Method: Practices were randomly assigned to receive recommendations for follow-up investigations for cancer (FHT cancer module) or the active control. Algorithms were applied to the electronic medical record, and used demographic information and abnormal test results that are associated with a risk of undiagnosed cancer (that is, anaemia/iron deficiency, thrombocytosis, and raised prostate-specific antigen) to identify patients requiring further investigation and provide recommendations for care. The intervention consisted of the FHT cancer module, a case-based learning series, and ongoing practice support. Using the intention-to-treat approach, the between-arm difference in the proportion of patients with abnormal test results who were followed up according to guidelines was determined at 12 months.
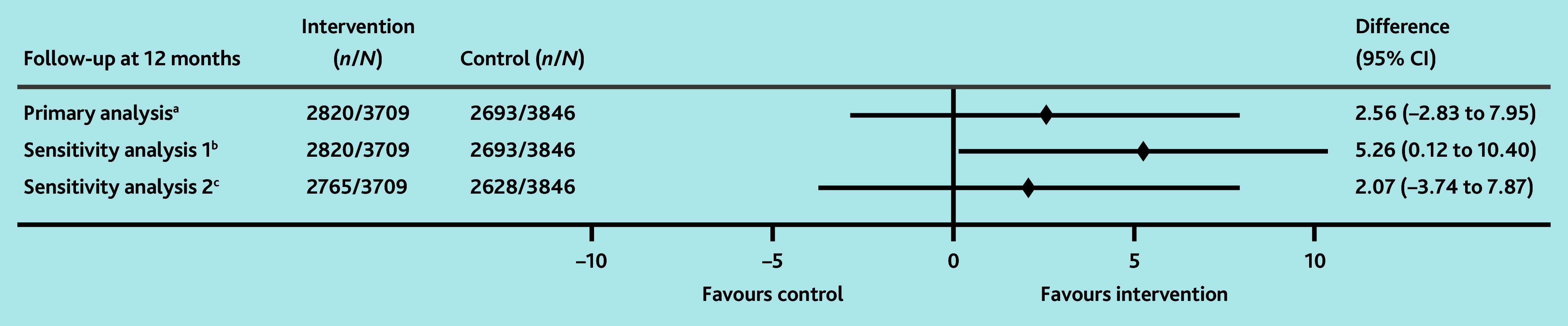
Results: In total, 7555 patients were identified as at risk of undiagnosed cancer. At 12 months post-randomisation, 76.0% of patients in the intervention arm had received recommended follow-up (21 practices, n = 2820/3709), compared with 70.0% in the control arm (19 practices, n = 2693/3846; estimated between-arm difference = 2.6% [95% confidence interval (CI)] = -2.8% to 7.9%; odds ratio = 1.15 [95% CI = 0.87 to 1.53]; P = 0.332).
Conclusion: The FHT cancer module intervention did not increase the proportion of patients receiving guideline-concordant care. The proportion of patients receiving recommended follow-up was high, suggesting a possible ceiling effect for the intervention.
Keywords: cancer; clinical decision support; diagnosis; general practice; primary care.
© The Authors.
Conflict of interest statement
The FHT software was developed by the University of Melbourne in collaboration with Western Health. These affiliations were displayed on the FHT dashboard and training materials. Craig Nelson, Jon Emery, and Jo-Anne Manski-Nankervis are the co-leads of the FHT programme, and Douglas Boyle leads the technical team that developed the software. Intellectual property related to FHT is owned by the University of Melbourne.
Figures
Similar articles
-
Effectiveness of Electronic Quality Improvement Activities to Reduce Cardiovascular Disease Risk in People With Chronic Kidney Disease in General Practice: Cluster Randomized Trial With Active Control.JMIR Form Res. 2025 Feb 3;9:e54147. doi: 10.2196/54147. JMIR Form Res. 2025. PMID: 39899838 Free PMC article. Clinical Trial.
-
Clinical Acceptability of a Quality Improvement Program for Reducing Cardiovascular Disease Risk in People With Chronic Kidney Disease in Australian General Practice: Qualitative Study.JMIR Hum Factors. 2024 Nov 13;11:e55667. doi: 10.2196/55667. JMIR Hum Factors. 2024. PMID: 39535290 Free PMC article.
-
Optimising a clinical decision support tool to improve chronic kidney disease management in general practice.BMC Prim Care. 2024 Jun 19;25(1):220. doi: 10.1186/s12875-024-02470-w. BMC Prim Care. 2024. PMID: 38898462 Free PMC article.
-
Improving the referral process for familial breast cancer genetic counselling: findings of three randomised controlled trials of two interventions.Health Technol Assess. 2005 Feb;9(3):iii-iv, 1-126. doi: 10.3310/hta9030. Health Technol Assess. 2005. PMID: 15694064 Review.
-
Behavioural modification interventions for medically unexplained symptoms in primary care: systematic reviews and economic evaluation.Health Technol Assess. 2020 Sep;24(46):1-490. doi: 10.3310/hta24460. Health Technol Assess. 2020. PMID: 32975190 Free PMC article.
Cited by
-
Implementation of a Quality Improvement and Clinical Decision Support Tool for Cancer Diagnosis in Primary Care: Process Evaluation.JMIR Cancer. 2025 Jun 12;11:e65461. doi: 10.2196/65461. JMIR Cancer. 2025. PMID: 40505100 Free PMC article. Clinical Trial.
-
Pancreatic Cancer Risk Assessment Tools in Primary Care: A Mixed Methods Systematic Review.J Gastrointest Cancer. 2025 Jun 5;56(1):128. doi: 10.1007/s12029-025-01229-5. J Gastrointest Cancer. 2025. PMID: 40471466 Free PMC article.
References
-
- Emery JD. The challenges of early diagnosis of cancer in general practice. Med J Aust. 2015;203(10):391–393. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical