

Bias and negative values of COVID-19 vaccine effectiveness estimates from a test-negative design without controlling for prior SARS-CoV-2 infection
- PMID: 39567531
- PMCID: PMC11579392
- DOI: 10.1038/s41467-024-54404-w
Bias and negative values of COVID-19 vaccine effectiveness estimates from a test-negative design without controlling for prior SARS-CoV-2 infection
Abstract
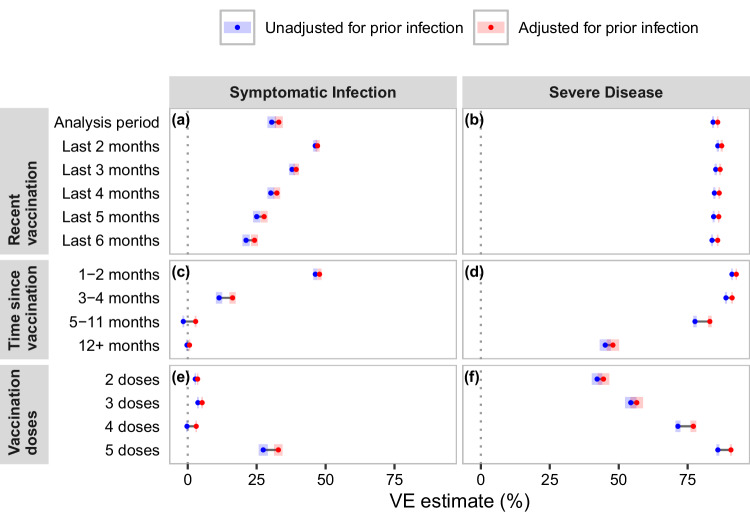
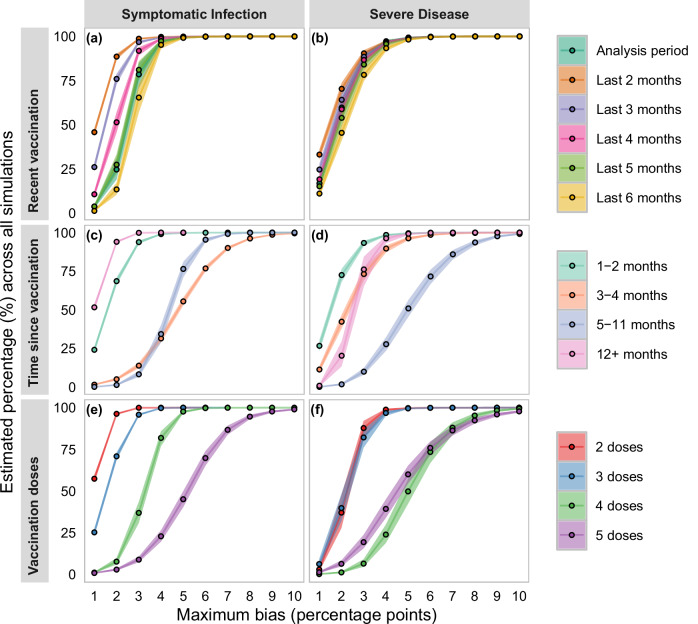
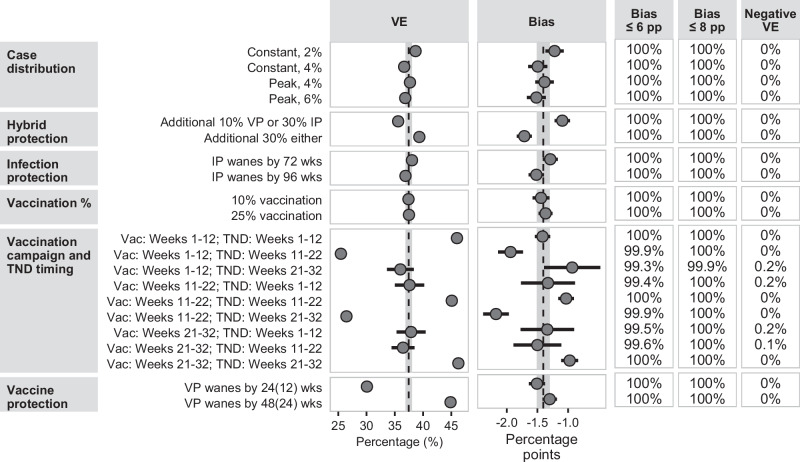
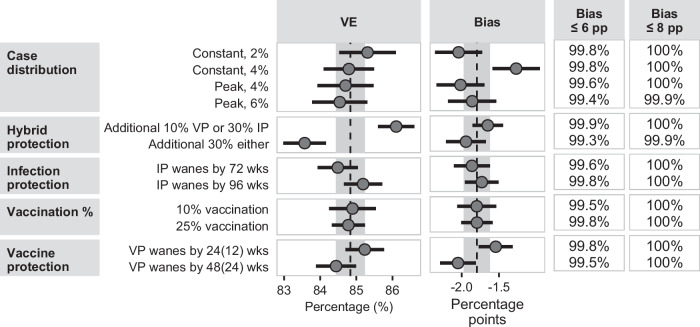
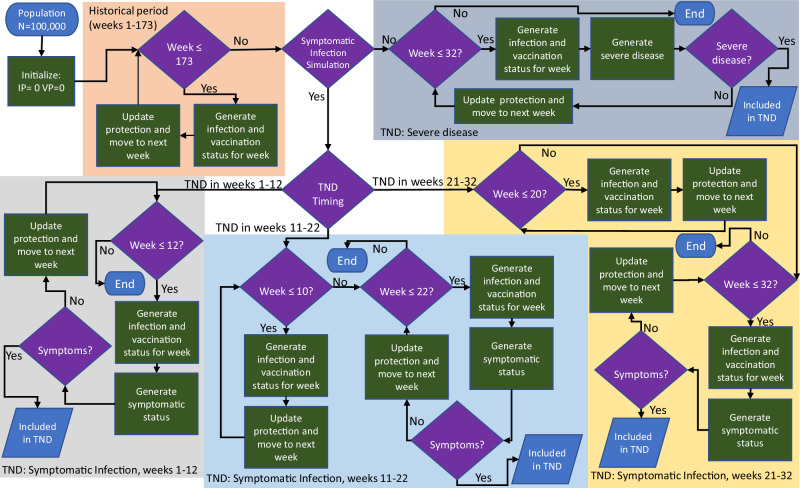
Test-negative designs (TNDs) are used to assess vaccine effectiveness (VE). Protection from infection-induced immunity may confound the association between case and vaccination status, but collecting reliable infection history can be challenging. If vaccinated individuals have less infection-induced protection than unvaccinated individuals, failure to account for infection history could underestimate VE, though the bias is not well understood. We simulated individual-level SARS-CoV-2 infection and COVID-19 vaccination histories and a TND. VE against symptomatic infection and VE against severe disease estimates unadjusted for infection history underestimated VE compared to estimates adjusted for infection history, and unadjusted estimates were more likely to be below 0%, which could lead to an incorrect interpretation that COVID-19 vaccines are harmful. TNDs assessing VE immediately following vaccine rollout introduced the largest bias and potential for negative VE against symptomatic infection. Despite the potential for bias, VE estimates from TNDs without prior infection information are useful because underestimation is rarely more than 8 percentage points.
© 2024. This is a U.S. Government work and not under copyright protection in the US; foreign copyright protection may apply.
Conflict of interest statement
Competing interests: The authors declare that they do not have any commercial or other associations that might pose a conflict of interest.
Figures
References
-
- Link-Gelles, R. et al. Early estimates of bivalent mRNA booster dose vaccine effectiveness in preventing symptomatic SARS-CoV-2 infection attributable to omicron BA.5– and XBB/XBB.1.5–related sublineages among immunocompetent adults—increasing community access to testing program, United States. MMWR Morb. Mortal. Wkly. Rep.72, 119–124 (2023). - DOI - PMC - PubMed
-
- Tenforde, M. W. et al. Early estimates of bivalent mRNA vaccine effectiveness in preventing COVID-19–associated emergency department or urgent care encounters and hospitalizations among immunocompetent adults—VISION network, nine states. MMWR Morb. Mortal. Wkly. Rep.71, 1616–1624 (2022). - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
