

Genetic and phenotypic architecture of human myocardial trabeculation
- PMID: 39567769
- PMCID: PMC11634767
- DOI: 10.1038/s44161-024-00564-3
Genetic and phenotypic architecture of human myocardial trabeculation
Abstract
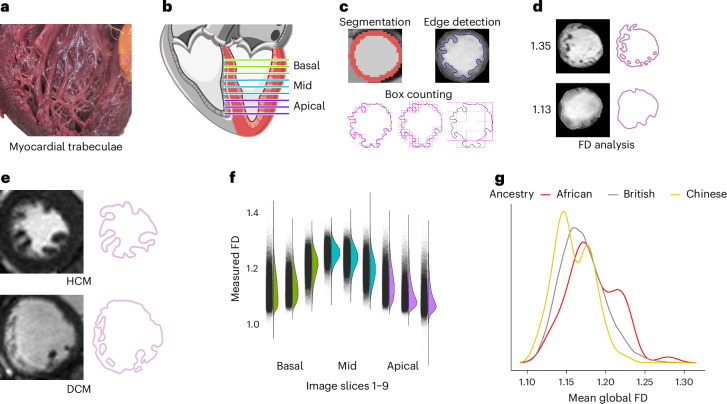
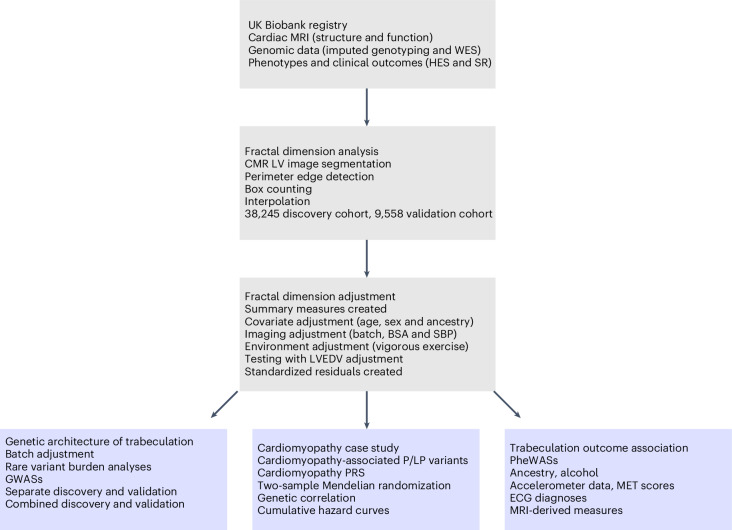
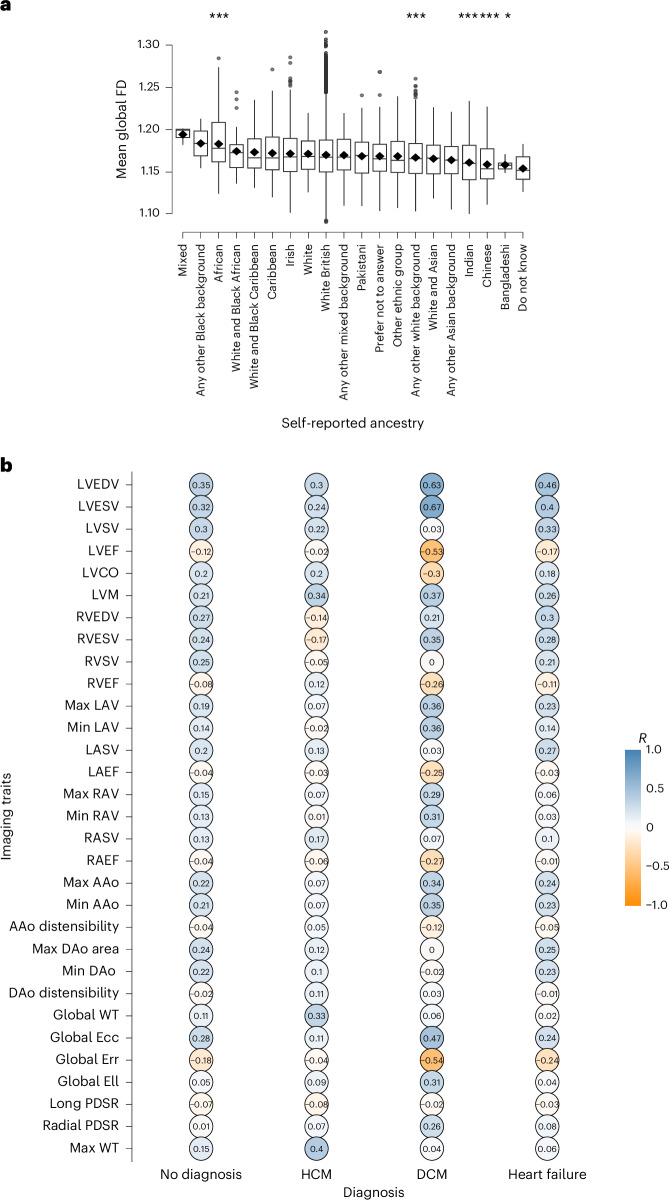
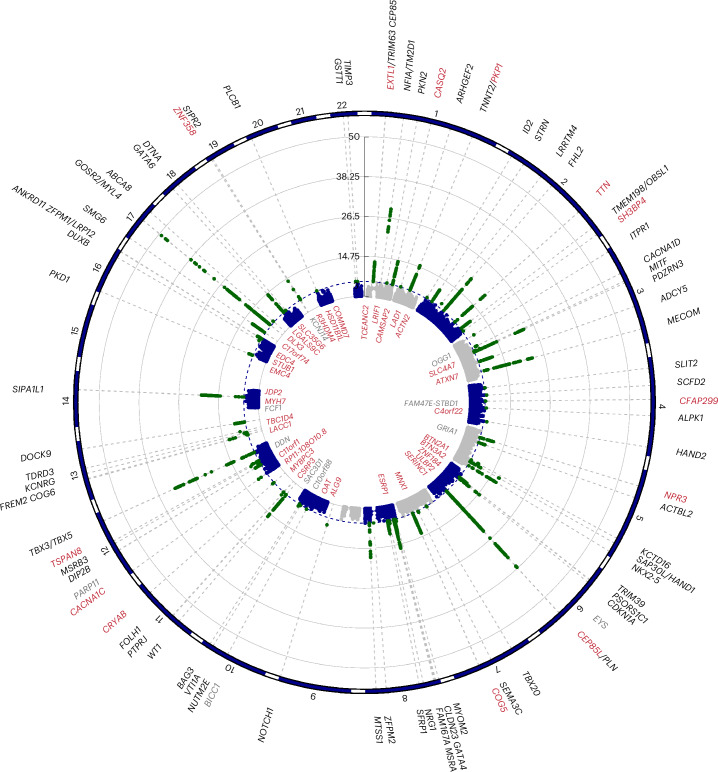
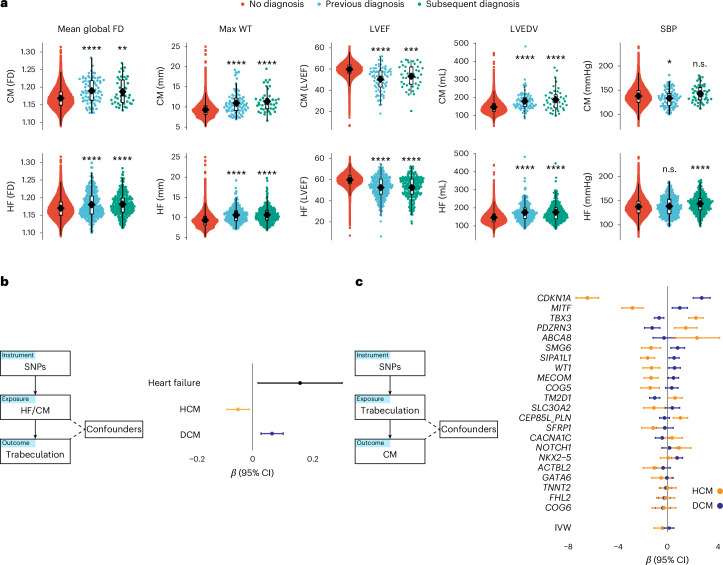
Cardiac trabeculae form a network of muscular strands that line the inner surfaces of the heart. Their development depends on multiscale morphogenetic processes and, while highly conserved across vertebrate evolution, their role in the pathophysiology of the mature heart is not fully understood. Here we report variant associations across the allele frequency spectrum for trabecular morphology in 47,803 participants of the UK Biobank using fractal dimension analysis of cardiac imaging. We identified an association between trabeculation and rare variants in 56 genes that regulate myocardial contractility and ventricular development. Genome-wide association studies identified 68 loci in pathways that regulate sarcomeric function, differentiation of the conduction system and cell fate determination. We found that trabeculation-associated variants were modifiers of cardiomyopathy phenotypes with opposing effects in hypertrophic and dilated cardiomyopathy. Together, these data provide insights into mechanisms that regulate trabecular development and plasticity, and identify a potential role in modifying monogenic disease expression.
© 2024. The Author(s).
Conflict of interest statement
Competing interests: D.P.O. has consulted for Bayer AG and Bristol-Myers Squibb. J.S.W. has consulted for MyoKardia, Inc., Pfizer, Foresite Labs, Health Lumen and Tenaya Therapeutics and has received research support from Bristol-Myers Squibb. R.T.L. has consulted for Health Lumen and FITFILE. None of these activities are directly related to the work presented here. The other authors declare no competing interests.
Figures











References
-
- Monte-Nieto, G. et al. Control of cardiac jelly dynamics by NOTCH1 and NRG1 defines the building plan for trabeculation. Nature557, 439–445 (2018). - PubMed
-
- Walsh, R. The trouble with trabeculation: how genetics can help to unravel a complex and controversial phenotype. J. Cardiovasc. Transl. Res.16, 1310–1324 (2023). - PubMed
MeSH terms
Grants and funding
- [107469/Z/15/Z/Wellcome Trust (Wellcome)
- RG/F/22/110078/British Heart Foundation (BHF)
- RG/19/6/34387/British Heart Foundation (BHF)
- CH/F/24/90015/BHF_/British Heart Foundation/United Kingdom
- 5R01HL167509-02/Foundation for the National Institutes of Health (Foundation for the National Institutes of Health, Inc.)
- R01 HL167509/HL/NHLBI NIH HHS/United States
- FS/IPBSRF/22/27059/British Heart Foundation (BHF)
- CH/P/23/80008/British Heart Foundation (BHF)
- MC_UP_1605/13/RCUK | Medical Research Council (MRC)
- EP/W01842X/1/RCUK | Engineering and Physical Sciences Research Council (EPSRC)
- 21JTA/Sir Jules Thorn Charitable Trust
- WT_/Wellcome Trust/United Kingdom
LinkOut - more resources
Full Text Sources