

Tailored bi-atrial linear ablation guided by electrophysiological mapping for persistent atrial fibrillation
- PMID: 39567904
- PMCID: PMC11577918
- DOI: 10.1186/s12872-024-04332-w
Tailored bi-atrial linear ablation guided by electrophysiological mapping for persistent atrial fibrillation
Abstract
Aim: To explore the safety and efficacy of a novel strategy (bi-atrial linear catheter ablation guided by electrophysiological mapping) for persistent atrial fibrillation (PeAF) treatment.
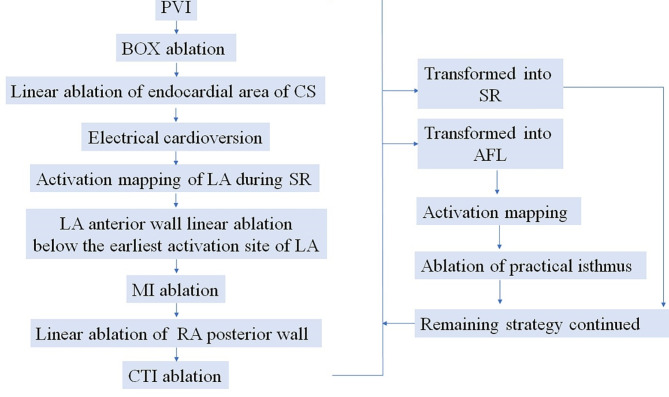
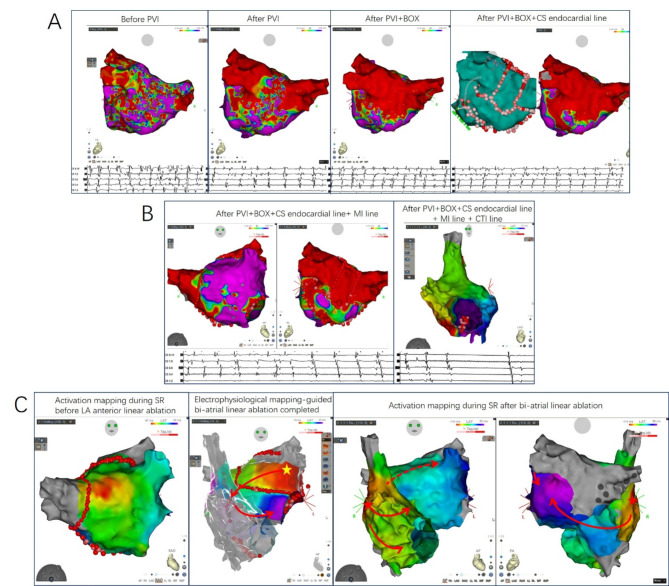
Methods: 83 patients with PeAF were enrolled for evaluation of ablation strategy. 43 patients were subjected to pulmonary vein isolation (PVI) strategy (PVI group). 40 patients were subjected to bi-atrial linear ablation strategy guided by electrophysiological mapping (PVI, left atrial BOX ablation, coronary sinus endocardial linear ablation, tailored left atrial anterior wall linear ablation, mitral isthmus linear ablation with necessary ethanol infusion into the vein of Marshall, right atrial posterior wall linear ablation and cavo-tricuspid isthmus ablation) (linear ablation group). Patients were followed up every 3 months.
Results: During a median follow-up of 12 (4-16) months, freedom from atrial fibrillation/atrial tachycardia recurrence was 87.5% in the linear ablation group and 65.1% in the PVI group (P < 0.01). A Cox regression multivariate analysis revealed that ablation strategy group (tailored bi-atrial linear ablation) (HR 0.33, 95% CI 0.12-0.91, P = 0.03) was the only independent predictor of recurrence.
Conclusion: Tailored bi-atrial linear ablation strategy guided by electrophysiological mapping resulted in improved outcomes without compromising safety for patients with PeAF.
Keywords: Catheter ablation; Electrophysiological mapping guidance; Linear ablation; Persistent atrial fibrillation.
© 2024. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: The present study was preapproved by the Research Development and Human Ethics Committee of the First Affiliated Hospital of Dalian Medical University. The need for written informed consent was waived by the Human Ethics Committee of the First Affiliated Hospital of Dalian Medical University due to retrospective nature of the study. All methods were performed in accordance with the Declaration of Helsinki. Consent for publication: Not Applicable. Competing interests: The authors have no relevant financial or non-financial interests to disclose. The content of this manuscript has been presented [Abstract] at the [HRS 2024], [Heart Rhythm, Vol. 5, May Supplement 2024, S1-S772].
Figures




Similar articles
-
Single-center experience of the FIRM technique to ablate paroxysmal and persistent atrial fibrillation.J Cardiovasc Electrophysiol. 2019 Apr;30(4):493-502. doi: 10.1111/jce.13832. Epub 2019 Jan 8. J Cardiovasc Electrophysiol. 2019. PMID: 30580474
-
Comparison of the empirical linear ablation and low voltage area-guided ablation in addition to pulmonary vein isolation in patients with persistent atrial fibrillation: a propensity score-matched analysis.BMC Cardiovasc Disord. 2022 Jan 22;22(1):13. doi: 10.1186/s12872-022-02460-9. BMC Cardiovasc Disord. 2022. PMID: 35065605 Free PMC article.
-
Efficacy of Left Atrial Voltage-Based Catheter Ablation of Persistent Atrial Fibrillation.J Cardiovasc Electrophysiol. 2016 Sep;27(9):1055-63. doi: 10.1111/jce.13019. Epub 2016 Jun 30. J Cardiovasc Electrophysiol. 2016. PMID: 27235000
-
Impact of targeting adenosine-induced transient venous reconnection in patients undergoing pulmonary vein isolation for atrial fibrillation: a meta-analysis of 3524 patients.J Cardiovasc Med (Hagerstown). 2017 Jul;18(7):478-489. doi: 10.2459/JCM.0000000000000408. J Cardiovasc Med (Hagerstown). 2017. PMID: 28514791 Review.
-
Catheter Ablation for Long-Standing Persistent Atrial Fibrillation.Methodist Debakey Cardiovasc J. 2015 Apr-Jun;11(2):87-93. doi: 10.14797/mdcj-11-2-87. Methodist Debakey Cardiovasc J. 2015. PMID: 26306125 Free PMC article. Review.
References
-
- Terricabras M, Verma A. Is pulmonary vein isolation enough for persistent atrial fibrillation? J Cardiovasc Electrophysiol. 2020;31(8):2148–53. - PubMed
-
- Gianni C, Mohanty S, Di Biase L, Metz T, Trivedi C, Gokoglan Y, Gunes MF, Bai R, Al-Ahmad A, Burkhardt JD, et al. Acute and early outcomes of focal impulse and rotor modulation (FIRM)-guided rotors-only ablation in patients with nonparoxysmal atrial fibrillation. Heart Rhythm. 2016;13(4):830–5. - PubMed
-
- Verma A, Jiang CY, Betts TR, Chen J, Deisenhofer I, Mantovan R, Macle L, Morillo CA, Haverkamp W, Weerasooriya R, et al. Approaches to catheter ablation for persistent atrial fibrillation. N Engl J Med. 2015;372(19):1812–22. - PubMed
-
- Park I, Jeong DS, Park SJ, Ahn JH, Kim J, Kim EK, Sung K, Kim WS, Park PW. Impact of maze procedure in patients with severe tricuspid regurgitation and persistent atrial fibrillation. J Thorac Cardiovasc Surg 2021. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
