

Fetal rotation examined with ultrasound in a sub-Saharan population: A longitudinal cohort study
- PMID: 39568051
- PMCID: PMC11683555
- DOI: 10.1111/aogs.15013
Fetal rotation examined with ultrasound in a sub-Saharan population: A longitudinal cohort study
Abstract
Introduction: Occiput posterior (OP) position rates at birth are 5%-8% in studies mainly comprising white European women. The anthropoid pelvis is common in black African women. This pelvic shape has a narrow anterior segment and an ample room posteriorly. The fetal head is wider posteriorly, and the OP position may be favorable in women with an anthropoid pelvic shape. We aimed to examine the fetal rotation with ultrasound longitudinally during the active phase of labor in a sub-Saharan population. We also aimed to examine associations between fetal position, delivery mode, and duration of labor.
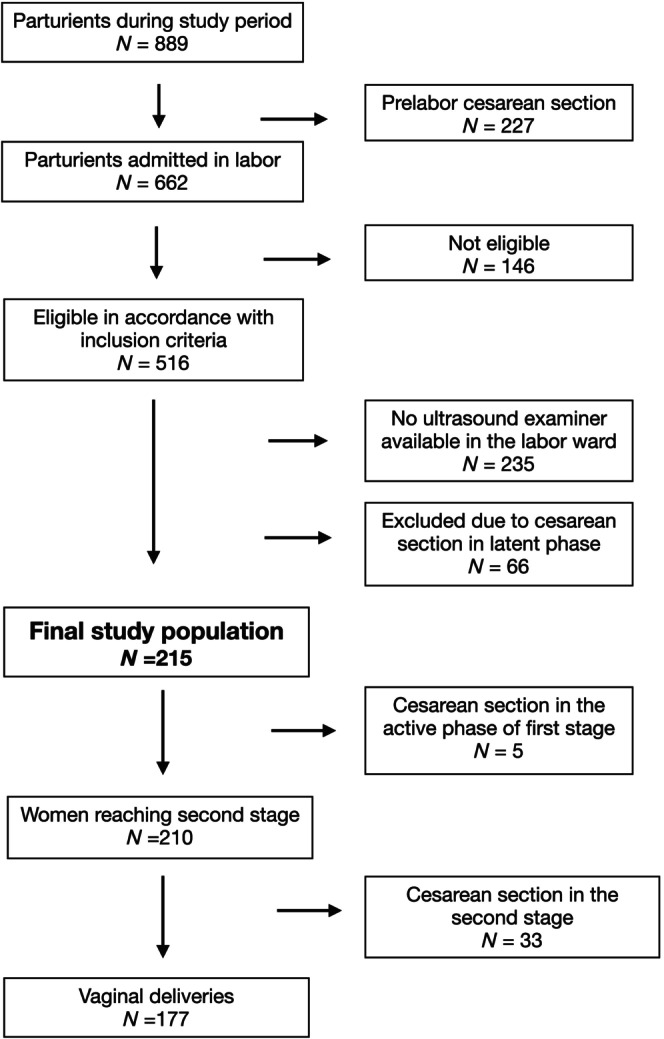
Material and methods: The study was conducted at Kilimanjaro Christian Medical Centre in Moshi, Tanzania from the 19th of November 2023 to 13th of April 2024. Women with a single fetus in cephalic presentation, gestational age >37 weeks, without previous or pre-labor cesarean section were eligible. Fetal position was classified as occiput anterior (OA) from 10 to 2 o'clock, occiput transverse (OT) at 3 or 9 o'clock, and OP position from 4 to 8 o'clock.
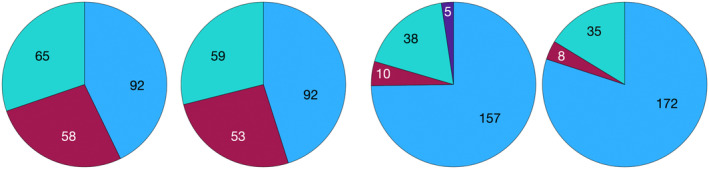
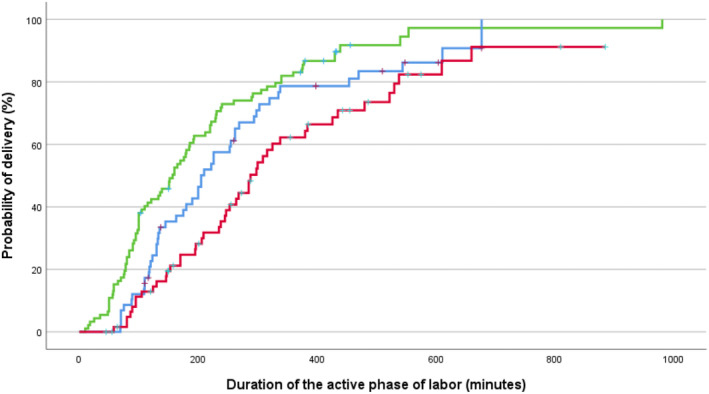
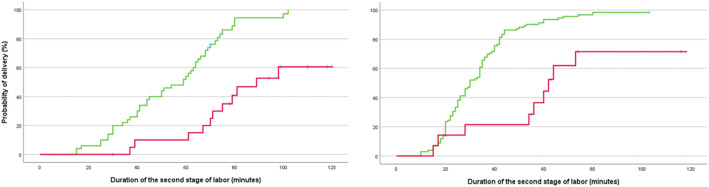
Results: The study participants comprised 215 women. Fetal positions at admission, in the first and second stage of labor and at birth are presented in the graphical figure. In all, 65/215 (30.2%) fetuses were in OP position at admission, 59/204 (28.9%) in the first stage, 38/210 (18.1%) in the second stage and 35/215 (16.3%) were delivered in OP position. The OP rates at birth were 25/92 (27.2%) in nulliparous and 10/123 (8.1%) in parous women. The operative delivery rate was 10/157 (6.4%) in women with ultrasound assessed fetal position as OA in the second stage (six cesarean section and four vacuum extractions), and 28/48 (58.3%) in the non-OA group (27 cesarean section and one vacuum extraction) (p < 0.01). The hazard ratio for delivery in the second stage was 0.26 (95% CI 0.13-0.52) for the non-OA vs the OA group in nulliparous women and 0.25 (95% CI 0.12-0.52) in parous women.
Conclusions: The persistent OP position rate at birth was higher than previously reported, and the operative intervention rate was nine time higher in women with the fetus in non-OA vs OA position in the second stage.
Keywords: birth; cesarean; maternity care; obstetrics; ultrasound.
© 2024 The Author(s). Acta Obstetricia et Gynecologica Scandinavica published by John Wiley & Sons Ltd on behalf of Nordic Federation of Societies of Obstetrics and Gynecology (NFOG).
Conflict of interest statement
The authors report no conflict of interest.
Figures
References
-
- Akmal S, Tsoi E, Howard R, Osei E, Nicolaides KH. Investigation of occiput posterior delivery by intrapartum sonography. Ultrasound Obstet Gynecol. 2004;24:425‐428. - PubMed
-
- Gardberg M, Laakkonen E, Salevaara M. Intrapartum sonography and persistent occiput posterior position: a study of 408 deliveries. Obstet Gynecol. 1998;91:746‐749. - PubMed
-
- Hjartardottir H, Lund SH, Benediktsdottir S, Geirsson RT, Eggebo TM. When does fetal head rotation occur in spontaneous labor at term: results of an ultrasound‐based longitudinal study in nulliparous women. Am J Obstet Gynecol. 2021;224(514):514.e1‐514.e9. - PubMed
-
- Torkildsen EA, Salvesen KA, Vonb P, Eggebo TM. Predictive value of ultrasound assessed fetal head position in primiparous women with prolonged first stage of labor. Acta Obstet Gynecol Scand. 2012;91:1300‐1305. - PubMed
-
- Hjartardottir H, Lund SH, Benediktsdottir S, Geirsson RT, Eggebo TM. Can ultrasound on admission in active labor predict labor duration and a spontaneous delivery? Am J Obstet Gynecol MFM. 2021;3:100383. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
