

Exploring the genetics of airflow limitation in lung function across the lifespan - a polygenic risk score study
- PMID: 39568778
- PMCID: PMC11577569
- DOI: 10.1016/j.eclinm.2024.102731
Exploring the genetics of airflow limitation in lung function across the lifespan - a polygenic risk score study
Abstract
Background: Chronic obstructive pulmonary disease (COPD) is caused by interactions between many factors across the life course, including genetics. A proportion of COPD may be due to reduced lung growth in childhood. We hypothesized that a polygenic risk score (PRS) for COPD is associated with lower lung function already in childhood and up to adulthood.
Methods: A weighted PRS was calculated based on the 82 association signals (p ≤ 5 × 10-8) revealed by the largest GWAS of airflow limitation (defined as COPD) to date. This PRS was tested in association with lung function measures (FEV1, FVC, and FEV1/FVC) in subjects aged 4-50 years from 16 independent cohorts participating in the Chronic Airway Diseases Early Stratification (CADSET) Clinical Research Collaboration. Age-stratified meta-analyses were conducted combining the results from each cohort (n = 45,406). These findings were validated in subjects >50 years old.
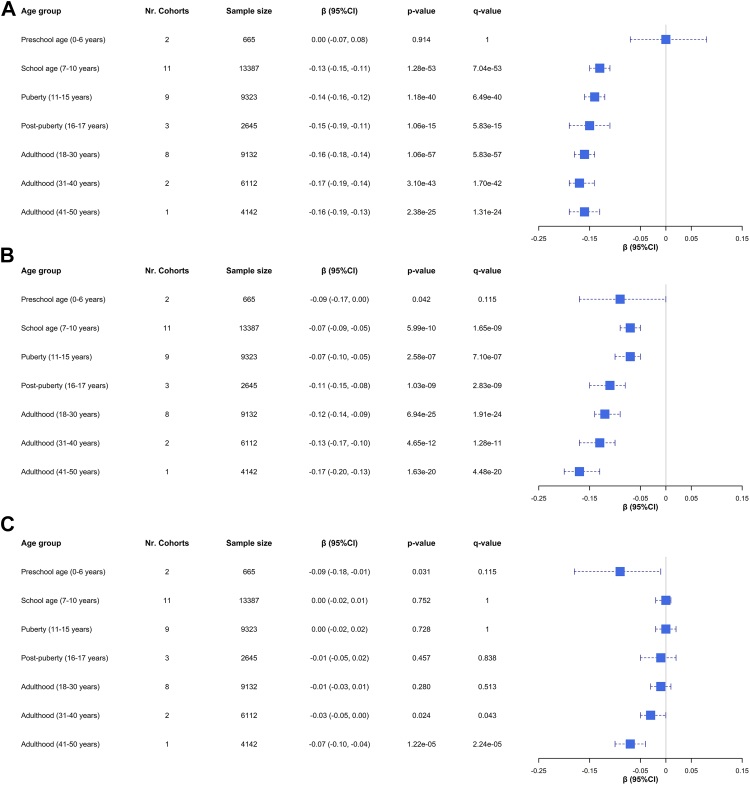
Findings: We found significant associations between the PRS for airflow limitation and: (1) lower pre-bronchodilator FEV1/FVC from school age (7-10 years; β: -0.13 z-scores per one PRS z-score increase [-0.15, -0.11], q-value = 7.04 × 10-53) to adulthood (41-50 years; β: -0.16 [-0.19, -0.13], q-value = 1.31 × 10-24); and (2) lower FEV1 (from school age: 7-10 years; β: -0.07 [-0.09, -0.05], q-value = 1.65 × 10-9, to adulthood: 41-50 years; β: -0.17 [-0.20, -0.13], q-value = 4.48 x 10-20). No effect modification by smoking, sex, or a diagnosis of asthma was observed.
Interpretation: We provide evidence that a higher genetic risk for COPD is linked to lower lung function from childhood onwards.
Funding: This study was supported by CADSET, a Clinical Research Collaboration of the European Respiratory Society.
Keywords: Chronic obstructive pulmonary disease; Genetics; Lung function; Polygenic risk score.
© 2024 The Author(s).
Conflict of interest statement
NH-P was supported with a Medium-Term Research Fellowship by the European Academy of Allergy and Clinical Immunology (EAACI) and a Long-Term Research Fellowship by the European Respiratory Society (ERS) (LTRF202101-00861), and lecture honoraria from OMNIPREX, S.L (outside of the submitted work). LLa was supported by the Fund for Scientific Research Flanders (Grant 3G037618), lecture honoraria from IPSA vzw, a non-profit organization facilitating lifelong learning for health care providers, and Chiesi; and consulting fees from AstraZeneca, all paid to the institution. LLa also declares unpaid membership of faculty board and faculty committees of the European Respiratory Society and Belgian Respiratory Society. LB received support from the K.G. Jebsen Center for Genetic Epidemiology funded by Stiftelsen Kristian Gerhard Jebsen; Faculty of Medicine and Health Sciences, NTNU; The Liaison Committee for Education, Research and Innovation in Central Norway; and the Joint Research Committee between St Olavs Hospital and the Faculty of Medicine and Health Sciences, NTNU. YS was supported by a grant from the China Scholarship Council. AL declares consulting fees regarding presentation of spirometry from Diagnostica Ltb and lecture honoraria from AstraZeneca, Boehringer Ingelheim, and GlaxoSmithKline. AC reports research grants funded by MRC, EPSRC, and Wellcome Trust; consulting fees from Worg Pharmaceuticals; lecture honoraria from GlaxoSmithKline, AstraZeneca, Stallergens-Greer, and Sanofi; and unpaid membership of a board of officers of the World Allergy Organization. GK was supported by grants from ZON-MW, Lung Foundation of the Netherlands, UBBO EMMIUS Foundation, GSK, Vertex, European Union (H2020 program), TEVA the Netherlands; consulting fees from AstraZeneca and PURE IMS; lecture fees from AstraZeneca, Boehringer Ingelheim and Sanofi; and participation as a chair at the exquAIro foundation (AI education for medicine and pharma). RF received funding from the European Research Council (ERC) under the European Union's Horizon 2020 research and innovation program (grant agreement No. 101044387), Instituto de Salud Carlos III (PI18/00018, PI21/00735), SEPAR and Serra Hunter Program. AA reports research grants, consulting fees, and lecture honoraria by GlaxoSmithKline, AstraZeneca, Menarini, Chiesi, and Sanofi; and unpaid roles as Chair Board of Directors of GOLD and Co-chair of CADSET. MS received funding from ERC under the European Union's Horizon 2020 research and innovation program (grant agreement No. 949906). EM is supported by grants from the EU (ERC, TRIBAL No 757919). EM also declares advisory board and lecture fees from ALK, AstraZeneca, and Chiesi outside the submitted work. The rest of the authors declare no conflicts of interest that might be perceived to influence the interpretation of this article.
Figures







































References
-
- Melén E., Faner R., Allinson J.P., et al. Lung-function trajectories: relevance and implementation in clinical practice. Lancet. 2024;403(10435):1494–1503. - PubMed
-
- Agusti A., Faner R. Lung function trajectories in health and disease. Lancet Respir Med. 2019;7(4):358–364. - PubMed
-
- Dharmage S.C., Bui D.S., Walters E.H., et al. Lifetime spirometry patterns of obstruction and restriction, and their risk factors and outcomes: a prospective cohort study. Lancet Respir Med. 2023;11(3) - PubMed
-
- Bui D.S., Lodge C.J., Burgess J.A., et al. Childhood predictors of lung function trajectories and future COPD risk: a prospective cohort study from the first to the sixth decade of life. Lancet Respir Med. 2018;6(7):535–544. - PubMed
-
- Belgrave D.C.M., Granell R., Turner S.W., et al. Lung function trajectories from pre-school age to adulthood and their associations with early life factors: a retrospective analysis of three population-based birth cohort studies. Lancet Respir Med. 2018;6(7):526–534. - PubMed
LinkOut - more resources
Full Text Sources
