

Clinical Presentations, Treatments, and Complications of Ileal Perforation at a Tertiary Center: A Cross-Sectional Study
- PMID: 39569228
- PMCID: PMC11578607
- DOI: 10.7759/cureus.72027
Clinical Presentations, Treatments, and Complications of Ileal Perforation at a Tertiary Center: A Cross-Sectional Study
Abstract
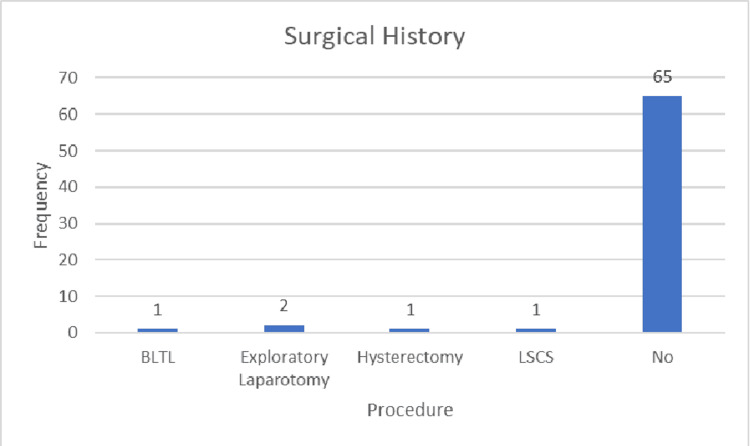
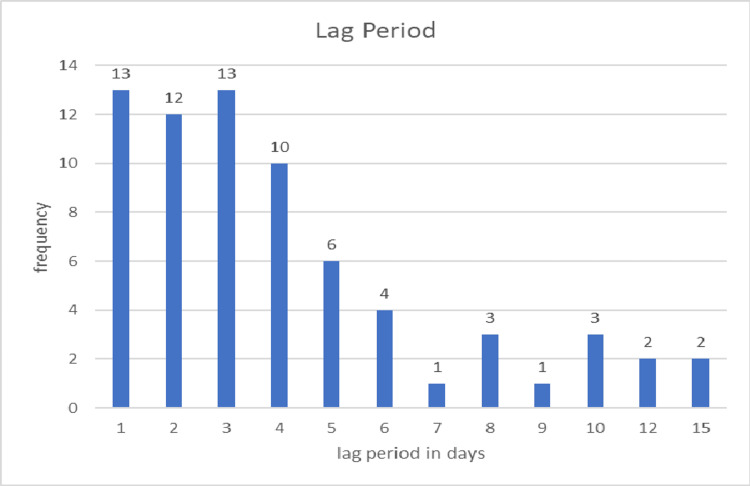
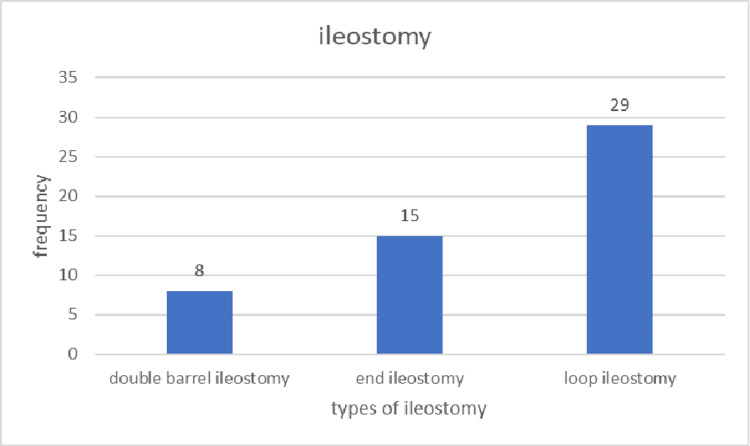
Background Ileal perforations represent one of the most common surgical emergencies in India, associated with significant morbidity and mortality rates. The causes of these perforations include infections such as tuberculosis and enteric fever, as well as malignancy and trauma. Management options encompass ileostomy, resection with anastomosis, and primary closure. Objective The objective of this study is to evaluate the clinical profile, etiology, management strategies, and complications associated with ileal perforation. Methodology A total of 70 patients with ileal perforation were included in the study. The proportions of various etiological factors, surgical interventions, and their associated complications were analyzed. The study aimed to determine whether ileostomy leads to fewer complications compared to primary repair. Results Ileal perforation is more prevalent in males than in females, with an incidence ratio of 2.68:1, predominantly affecting individuals in their 30s. Antituberculosis treatment does not consistently protect against perforation. Delays in presentation are linked to a higher likelihood of developing pyoperitoneum, increased chances of stoma creation (with a mean delay of 2.50 days in the closure group compared to 4.98 days in the ileostomy group), and greater mortality. Closure was performed in 18 patients (25.7%), while 52 patients (74.3%) underwent stoma creation. The duration of surgery was longer in the closure group (2.889 hours) than in the ileostomy group (2.635 hours) and also greater in the mortality group (three hours) compared to the non-mortality group (2.64 hours). The mean number of perforations was 1.59 ± 0.970, with 1.33 ± 0.840 in the closure group and 1.67 ± 1.004 in the ileostomy group. A higher number of perforations is associated with an increased likelihood of stoma creation. The most common cause of perforation was nonspecific, accounting for 40% of cases. The most frequently encountered complication was wound infection, occurring in 42.9% of patients. The mean duration of hospital stay was shorter in the ileostomy group (9.50 ± 5.500 days) than in the closure group (17.22 ± 19.219 days). Death occurred in 18.6% of cases, with higher rates observed in males (8:5), patients with delayed presentation, and elderly patients. A significant p-value was found in relation to leaks and fecal fistulas. Conclusions No significant difference was observed in complications associated with the various surgical procedures performed. However, a delay in presentation is linked to a higher rate of complications and increased mortality.
Keywords: enteric perforation; ileal perforation; ileostomy; pyoperitoneum; resection and anastomosis; stoma related complications; widal test.
Copyright © 2024, Ashok et al.
Conflict of interest statement
Human subjects: Consent for treatment and open access publication was obtained or waived by all participants in this study. Institutional Ethics Committee of Rajendra Institute of Medical Sciences issued approval MEMO NO. 48, date 16/02/2023. Animal subjects: All authors have confirmed that this study did not involve animal subjects or tissue. Conflicts of interest: In compliance with the ICMJE uniform disclosure form, all authors declare the following: Payment/services info: All authors have declared that no financial support was received from any organization for the submitted work. Financial relationships: All authors have declared that they have no financial relationships at present or within the previous three years with any organizations that might have an interest in the submitted work. Other relationships: All authors have declared that there are no other relationships or activities that could appear to have influenced the submitted work.
Figures





References
-
- Management of typhoid ileal perforation: a surgical experience of 44 cases. Ansari AG, Naqvi SQH, Ghumro AA, Jamali AH, Talpur AA. https://gjms.com.pk/index.php/journal/article/view/174 Gomal J Med Sci. 2009;7
-
- A study of 82 patients of non-traumatic terminal ileal perforation in Al-Kindy teaching hospital. Abdullah MS, Rassam RE, Almarzooq TJ. J Fac Med Baghdad. 2011;3:147–151.
LinkOut - more resources
Full Text Sources