

Complex regional pain syndrome after distal radius fracture: A survey of current practices
- PMID: 39570829
- PMCID: PMC11581307
- DOI: 10.1371/journal.pone.0314307
Complex regional pain syndrome after distal radius fracture: A survey of current practices
Abstract
Introduction: Complex regional pain syndrome (CRPS) is a common complication following distal radius fractures that is difficult to diagnose and can lead to permanent disability. While various proposed prophylaxis and treatment modalities exist, high-quality evidence guiding practice is limited. This survey of Orthopaedic Trauma Association (OTA) and Canadian Orthopaedic Association (COA) members was conducted with the primary aim of assessing practice patterns in distal radius fractures complicated with CRPS.
Methods: An electronic survey was distributed to practicing orthopaedic surgeons in the COA and OTA. Questions assessed practice setting, preference in management of distal radius fractures and CRPS, comfort level in managing CRPS, and identification of gaps in management. Responses were anonymized and collected over 8 months. Response data was analyzed using descriptive statistics; thematic analysis was used on free text response.
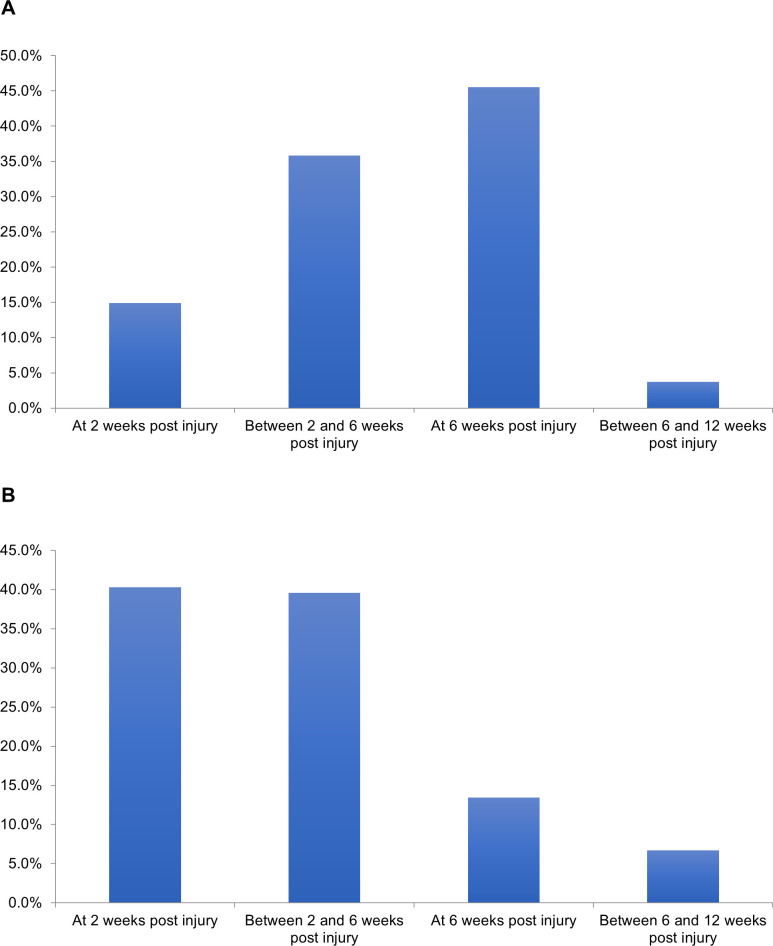
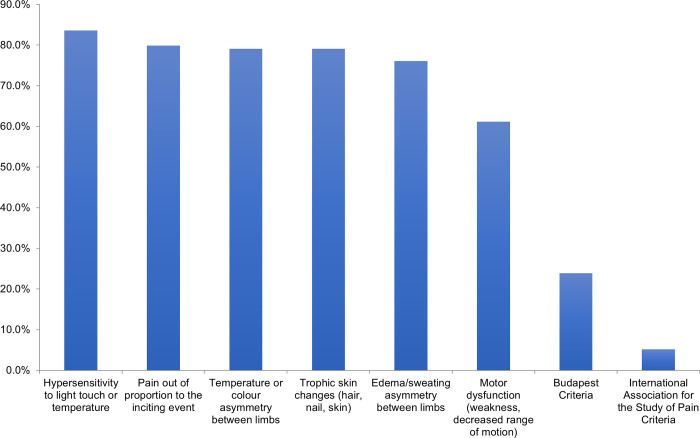
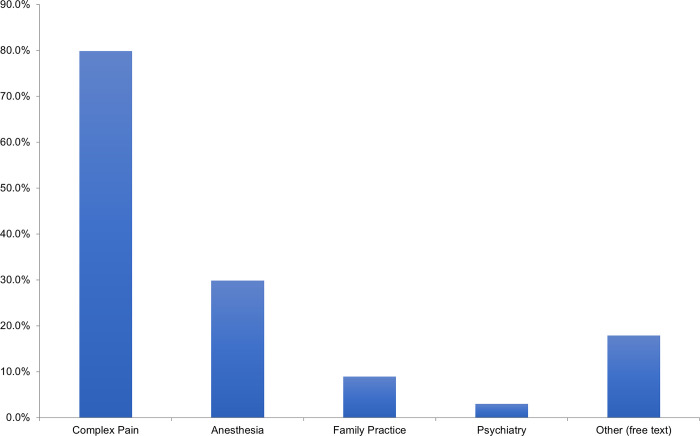
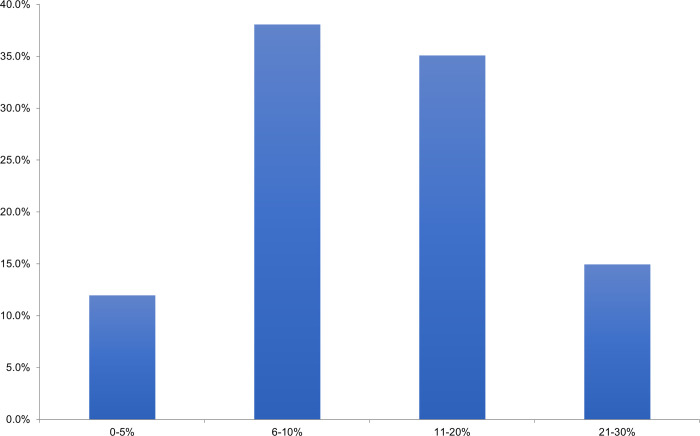
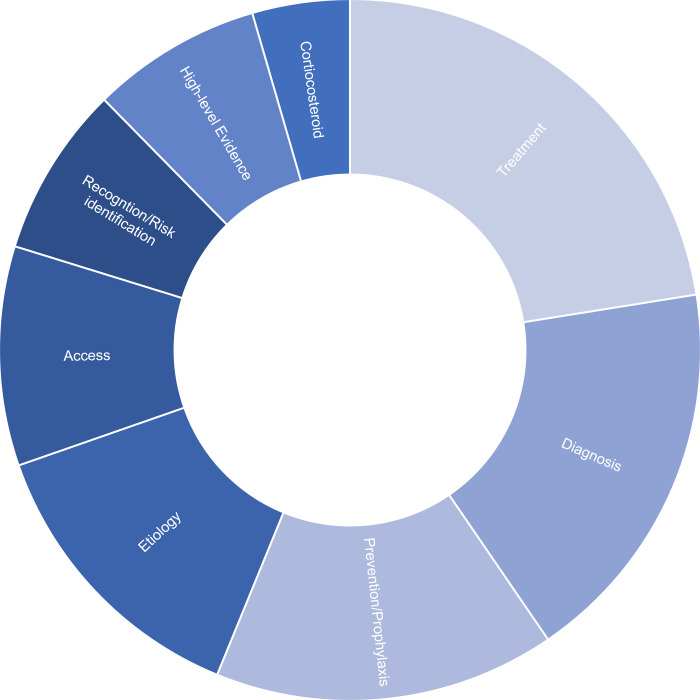
Results: 134 survey responses were completed. 84% of respondents felt the incidence of CRPS in distal radius fractures was 1-10%, while 15% felt it was closer to 11-20%. 24% of respondents utilized the "Budapest Criteria" to diagnose CRPS. 40% offered prophylaxis in patients felt to be at high risk of developing CRPS. 66% of surgeons felt neutral, uncomfortable, or very uncomfortable managing CRPS in distal radius fractures. When asked to consider adopting a prophylactic therapy, 38% of surgeons indicated that a therapy that reduced the absolute risk of CRPS by 6-10% would change their practice. Gaps in current practice included lack of evidence-based treatment and prevention strategies and diagnostic uncertainty.
Conclusion: This study identified that amongst orthopaedic surgeons in the COA and OTA, diagnosis, treatment, and prophylaxis strategies for CRPS in distal radius fractures are heterogeneous. Surgeons are not confident in their treatment of CRPS. Future studies using rigorous research methods are warranted to improve management.
Copyright: © 2024 Wang et al. This is an open access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
