

Nelarabine-combined chemotherapy improves outcome of T-cell acute lymphoblastic leukemia but shows more severe neurotoxicity: JALSG T-ALL213-O
- PMID: 39572007
- PMCID: PMC11786320
- DOI: 10.1111/cas.16405
Nelarabine-combined chemotherapy improves outcome of T-cell acute lymphoblastic leukemia but shows more severe neurotoxicity: JALSG T-ALL213-O
Abstract
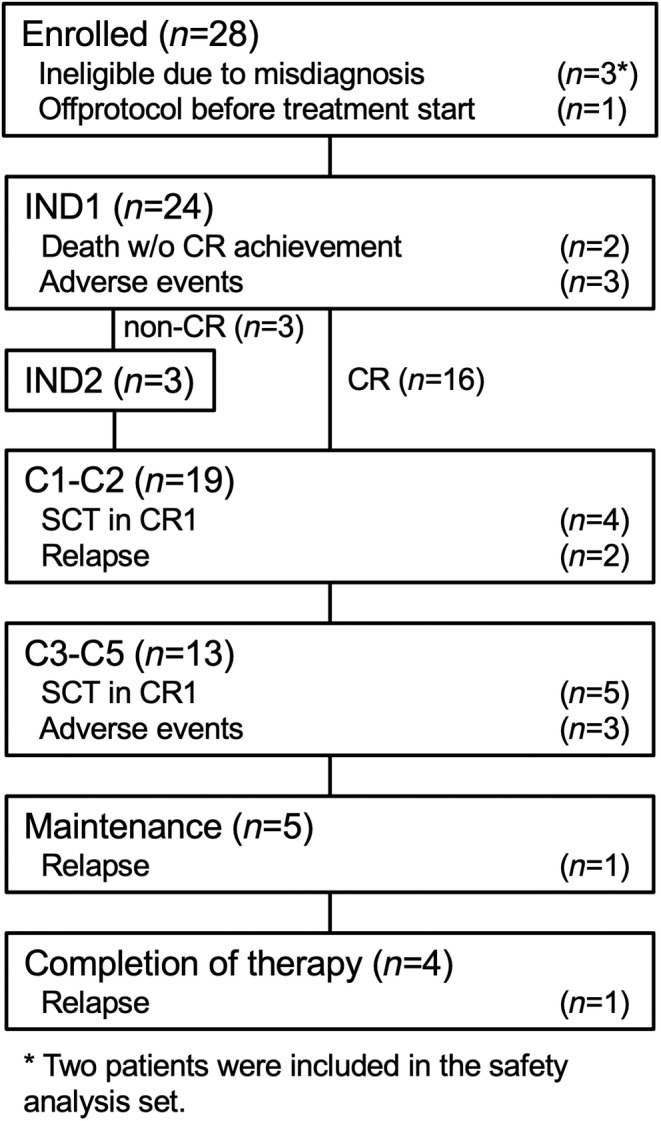
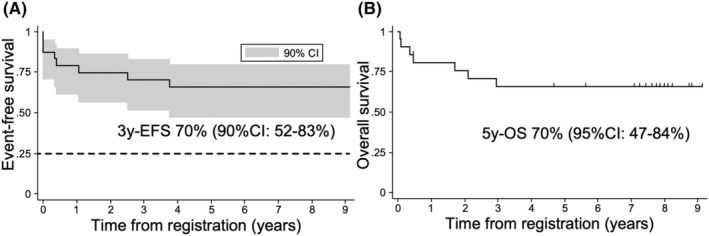
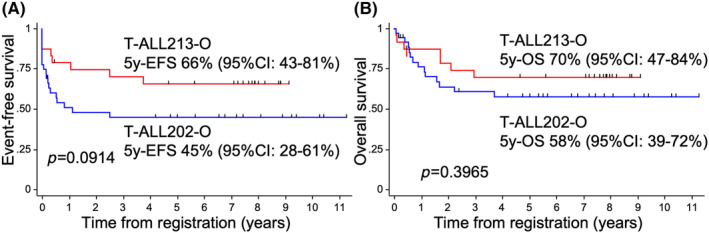
We investigated the effectiveness and safety of nelarabine (NEL)-combined chemotherapy for newly diagnosed adult T-cell acute lymphoblastic leukemia (T-ALL) patients. We conducted a phase II trial, T-ALL213-O, where adult T-ALL patients aged 25 to 64 were treated by a regimen based on that used in our previous study, ALL202-O. The main modifications from ALL202-O to T-ALL213-O were as follows: (1) NEL-combined chemotherapy, instead of consolidation (C)1, was used for non-complete remission (CR) patients after induction therapy (IND)1 as IND2; (2) NEL treatments were inserted into C3 and C5 on day 29. Twenty-four patients were analyzed. Ten patients did not receive NEL treatment due to therapy termination prior to C3. Three-year event-free survival (EFS) was 70%, with 52% as the lower limit of its 90% confidence interval, which exceeded the threshold of 25%; thus, the study treatment was considered effective. The CR rates by IND1, IND2, and both were 75%, 100%, and 88%, respectively. The 5-year EFS and 5-year overall survival rates were 66% and 70%, respectively, with median follow-ups of 7.7 and 7.8 years. The addition of NEL improved the CR rate but not survival, compared with T-ALL patients in ALL202-O. Severe neuropathy after NEL administration was observed at a high frequency. Seven (50%) of 14 patients treated with NEL showed grade 3 peripheral neuropathy and/or gait disturbance. The neurotoxicity was considered stronger than that previously reported. Combination therapy of NEL at this dose and intensive multidrug chemotherapy is associated with a high risk of severe neurotoxicity (JALSG T-ALL213-O, UMIN000010642).
Keywords: T‐ALL; acute lymphoblastic leukemia; clinical trial; nelarabine; neuropathy.
© 2024 The Author(s). Cancer Science published by John Wiley & Sons Australia, Ltd on behalf of Japanese Cancer Association.
Conflict of interest statement
Lecture fees: S.E. from Pfizer Inc., Novartis AG, and Janssen Pharmaceutical K.K.; M.I. from Pfizer Inc., Novartis AG, and Janssen Pharmaceutical K.K; M.Y. from Novartis AG and Nippon Shinyaku Co., Ltd. Research funds: M.I. from Novartis AG; K.H. from Kyowa Kirin Co., Ltd. Scholarship (incentive) endowments: M.I. from Kyowa Kirin Co., Ltd. and Nippon Shinyaku Co., Ltd.; K.H. from Kyowa Kirin Co., Ltd. K.H. is an editorial board member of
Figures
References
-
- Vadillo E, Dorantes‐Acosta E, Pelayo R, Schnoor M. T cell acute lymphoblastic leukemia (T‐ALL): new insights into the cellular origins and infiltration mechanisms common and unique among hematologic malignancies. Blood Rev. 2018;32:36‐51. - PubMed
-
- Huguet F, Chevret S, Leguay T, et al. Intensified therapy of acute lymphoblastic leukemia in adults: report of the randomized GRAALL‐2005 clinical trial. J Clin Oncol. 2018;36:2514‐2523. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
